3 Occupational performance and adaptation models
This chapter includes a number of models that address occupational therapy from the perspective articulated most prominently in North America. While occupational therapy grew out of both British and North American movements, the way that occupational therapy has been conceptualized in North America has had a widespread influence on theory throughout the world. While a number of different occupational performance models had been developed in different Western countries (e.g. the Canadian Occupational Performance Model (OPM) (DNHW & CAOT, 1983)), two have been selected to demonstrate different aspects of this approach. These are occupational performance models from the USA and Australia. The first two models presented in this chapter are the Occupational Performance (OP) model (Pedretti & Early, 2001), and with it the Occupational Therapy Practice Framework (OTPF) (AOTA, 2008), and the Occupational Performance Model (Australia) (OPMA) (Chapparo & Ranka, 1997). These models are most frequently, although not exclusively, used in physical rehabilitation practice because these models include a detailed focus on the body and its component capacities. In addition, a third model, the Occupational Adaptation (OA) model (first published: Schkade & Schultz, 1992), is presented.
The term occupational performance has been used widely in a range of occupational therapy publications, particularly in the late 1990s and early 2000s, and was often used interchangeably with other terms. As Christiansen and Baum (1997) explained, “The terms function or functional performance are often used in the medical literature to describe the ability of an individual to accomplish tasks of daily living. In an American Occupational Therapy Association (AOTA) position paper, Baum and Edwards (1995) observed that, when occupational therapists in the United States use the term function, they refer to an individual’s performance of activities, tasks and roles during daily occupations (occupational performance)” (p. 5).
Occupational Performance Model
In this chapter, once the Occupational Performance model, as it was presented by Pedretti and Early (2001), has been outlined, more recent developments are discussed in a section on the historical description of the model’s development. These include the Occupational Therapy Practice Framework (OTPF), first published in 2002 by the AOTA and now in its second edition (AOTA, 2008). While there are a range of occupational therapy models and frameworks published in the area of physical dysfunction, the OP model and the OTPF are both presented here because they flowed from or were associated with the official position of the AOTA (much of the Canadian work is discussed in Chapter 5). Pedretti’s and Early’s (2001) statement, “occupational performance terminology [used in the model] was defined and standardized in official documents of the AOTA” (p. 4) demonstrates that the OP model encapsulated the officially accepted view of the domain of concern of occupational therapy by the American Occupational Therapy Association at the time.
Main concepts and definitions of terms
Lorraine Williams Pedretti is the author most closely associated with articulating the OP model. She did not claim to have authored this model but explained that some components of the model “have always been the core of OT” (Pedretti & Early, 2001, p. 4) and other details were added by committees and task forces of the American Occupational Therapy Association during the 1970s. The diagram (1996, 2001) (see Figure 3.1) used to represent the model acknowledges that it is based on the uniform terminology for occupational therapists, which was published in three editions by the AOTA and was succeeded by the OTPF. Throughout the description of this model, the term patient is used, as that is the term most often used in relation to this model. That is, the model used the term patient to refer to the subject of therapy, and for consistency, we do the same.

As the name suggests, the central aim in this model is to facilitate occupational performance. Occupational performance was defined as, “the ability to perform those tasks that make it possible to carry out occupational roles in a satisfying manner appropriate for the individual’s developmental stage, culture, and environment” (Pedretti & Early, 2001, p. 5). Pedretti defined occupational roles as “the life roles that an individual holds in society” (1996, p. 3). Occupational roles develop in conjunction with the occupations in which people engage and include roles such as “pre-schooler, student, parent, homemaker, employee, volunteer, or retired worker” (2001, p. 5). Thus, the purpose of occupational performance is to be able to fulfil occupational roles.
The development of occupational performance is dependent upon sufficient opportunities to practice and learn the skills and abilities required to fulfil occupational roles and developmental tasks. The model provides a framework for aiding occupational therapists to systematically analyze the nature of the problems that are reducing the occupational performance of an individual. It comprises three elements: performance areas, performance components and performance contexts. The diagram provides the details of each of these elements and how they relate to occupational performance. Problems can arise that interfere with occupational performance. These problems might stem from “deficits in task learning experiences, performance components, or impoverished performance contexts” (Pedretti & Early, 2001, p. 5).
The performance areas are the first of the three elements described by the authors. The model outlines three performance areas into which activities are grouped. These are activities of daily living (ADL), work and productive activities, and play or leisure activities. Pedretti and Early (2001) explained, “ADL include the self-maintenance tasks of grooming, hygiene, dressing, feeding and eating, mobility, socialization, communication, and sexual expression. Work and productive activities include home management, care of others, educational activities, and vocational activities. Play and leisure include play exploration and play or leisure performance in age-appropriate activities.” (p. 5.) It appears that, by explaining the performance areas first, their connection to occupational performance and occupational roles could be emphasized. In addition, Pedretti and Early stated, “intervention strategies must ultimately be directed to the patient’s achievement in performance areas when a performance component (e.g. motor skill development) is being addressed” (p. 6). This emphasizes that, while the performance components provide details for occupational therapists that are particularly useful in planning rehabilitation interventions, occupational therapy intervention is for the purpose of enhancing the occupational performance required by an individual in each of the performance areas.
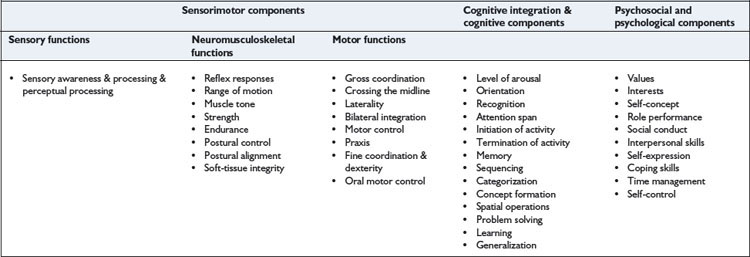
Performance components are “the learned developmental patterns of behaviour which are the substructure and foundation of the individual’s occupational performance” (Pedretti & Early, 2001, p. 5). The components of performance are categorized in the following three groups: sensorimotor, cognitive and cognitive integration, and psychosocial and psychological components. According to this model, “adequate neurophysiological development and integrated functioning of the performance components are basic to an individual’s ability to perform occupational tasks or activities in the performance areas” (pp. 5–6). The sensorimotor component includes three types of functions. These are sensory, neuromusculoskeletal and motor functions. The cognitive integration and cognitive components relate to the ability to use higher brain functions. The psychosocial and psychological components include those abilities required for social interaction and emotional processing. The model provides substantial detail about the nature of these performance components. These details have been listed in Table 3.1 for clarity.
The third element in the OP model is called performance contexts. The model acknowledges that occupational performance is conducted in a variety of contexts. Therefore, in order to gain a detailed understanding of an individual’s occupational performance, occupational therapists need to know both how the abilities of the individual affect his or her performance and how the context in which occupations are performed influence that performance. Performance contexts are conceptualized as temporal and environmental. Pedretti and Early (2001) listed the following as examples of the temporal context: “the individual’s age, developmental stage or phase of maturation, and stage in important life processes such as parenting, education, or career… [and] disability status (e.g., acute, chronic, terminal, improving, or declining) must also be considered” (p. 6). These examples suggest that, in this model, the temporal contexts appear to relate primarily to the individual.
Intervention
Underlying the model are two key approaches to facilitating occupational performance: remediation and compensation. In a remediation approach, intervention is targeted towards improving performance components, with the assumption that such improvements will lead to enhanced occupational performance in the performance areas. A compensatory approach is used when remediation is not considered achievable or feasible. According to Pedretti and Early (2001), the latter approach “focuses on remaining abilities and aims to improve function by adapting or compensating for performance component deficits” (p. 6). They proposed that examples of this approach might include adapting the methods used to perform tasks, providing assistive devices or modifying the environment.
The model outlines four levels of intervention. As the main focus of this model is remediation, the four levels primarily categorize methods that could be used for the remediation of problems in performance components. The levels in sequence are adjunctive methods, enabling activities, purposeful activity and occupations. They represent an intervention continuum that “takes the patient through a logical progression from dependence to occupational performance to resumption of valued social and occupational roles” (Pedretti & Early, 2001, p. 7). However, this continuum is not meant to be used in a strictly stepwise fashion and the various levels can overlap and be used simultaneously as required. Essentially, these intervention levels are based on the assumption that purposeful activity is the “primary treatment tool of occupational therapy” (p. 7) and that adjunctive methods and enabling activities are used as preparatory to functional activity in performance areas, rather than the aim of remediating problems in the performance components being an end in itself. As they stated, “exclusive use of such preparatory methods out of context of the patient’s occupational performance is not considered OT” (p. 7).
The first level of intervention is adjunctive methods. These are “procedures that prepare the patient for occupational performance but are preliminary to the use of purposeful activity” (p. 7). These methods generally focus on remediating performance components or maintaining structural integrity of body parts to prevent problems that could interfere with their potential use. They include methods such as “exercise, facilitation and inhibition techniques, positioning, sensory stimulation, selected physical agent modalities, and provision of devices such as braces and splints” (p. 7). Pedretti and Early (2001) emphasized that occupational therapists using these methods need to plan for progression to the subsequent intervention levels to ensure that adjunctive methods remain preparatory to purposeful activity.
The second level is enabling activities. This level involves the use of activities that might not be considered purposeful. Interventions at this level often involve simulation tasks, examples of which include “sanding boards, skate boards, stacking cones or blocks, practice boards for mastery of clothing fasteners and hardware, driving simulators, work simulators, and tabletop activities such as form boards for training in perceptual-motor skills” (Pedretti & Early, 2001, p. 7). These are often used when the requirements of purposeful activities are beyond the capabilities of patients. Essentially they represent graded activities that might enable patients to engage in activities for remediation and experience success, when purposeful activities would not be likely to result in this level of success. However, similar to adjunct methods, they need to be regarded as preparatory to purposeful activity. The primary goal of the first two levels of intervention is the remediation of performance components.
Pedretti and Early (2001) also included the use of equipment in this level. They listed equipment such as “wheelchairs, ambulatory aids, special clothing, communication devices, environmental control systems, and other assistive devices” (p. 7) as interventions at this level. It appears that their reason for including these devices here (rather than as environmental adaptations) could relate to purposeful activity being the main type of intervention proposed. As devices and equipment cannot be categorized as purposeful activity, they are probably conceptualized as tools for enabling performance, as are enabling activities. This approach appears to differ from some of the models presented in the following chapter, which present the environment as one of three primary intervention categories (i.e. person, environment, occupation).
The third intervention level is purposeful activity. Pedretti and Early (2001) emphasized that purposeful activity has always been at the core of occupational therapy. They defined purposeful activity as “activities that have an inherent or autonomous goal and are relevant and meaningful to the patient” (p. 8). It is the goal, relevance and meaningfulness to the patient that distinguishes this level from the second level, in which the activities chosen might have a goal that is meaningful to the occupational therapist but might not be evident to or valued by the client. The model assumes that activities become meaningful and purposeful to an individual because that individual needs them for functioning independently in their performance areas. Therefore, it is their contribution to the performance areas that makes activities purposeful.
At this level of intervention, purposeful activity is used for the purpose of “assessing and remediating deficits in the performance areas” (Pedretti & Early, 2001, p. 8). Thus, the focus is shifted to performance areas − compared with centring on performance components at the first two levels. Examples of the activities used are “feeding, hygiene, dressing, mobility, communication, arts, crafts, games, sports, work, and educational activities” (p. 8) and these could be conducted in the patient’s home, a community agency, or a healthcare facility.
Pedretti and Early (2001) identified two “intervention approaches” (p. 10) that are valuable to use in conjunction with the OP model in the area of physical dysfunction. These are the biomechanical and motor control models. Each of these models provides principles for the treatment of movement problems caused by different processes. The biomechanical model “applies the mechanical principles of kinetics and kinematics to the movement of the human body. These mechanical principles deal with the way that forces acting on the body affect movement and equilibrium.” (p. 10.) The biomechanical model guides the assessment and restoration of range of motion, muscle strength and endurance (muscular and cardiovascular) and the prevention and reduction of deformity. The biomechanical model is used for individuals with sensorimotor problems resulting from “motor unit or orthopaedic disorders but whose central nervous system (CNS) is intact” (p. 10). Common intervention methods include “joint measurement, muscle strength testing, kinetic activity, therapeutic exercise, and orthotics” (p. 10) and many of the common interventions from the first two levels (adjunctive methods and enabling activities) derive from the biomechanical model.
Second is the motor control model, which addresses CNS problems. Pedretti and Early (2001) identified four approaches within this model. These were the Rood and Brunnstrom approaches to movement therapy, Knott and Voss’s proprioceptive neuromuscular facilitation, and Bobath’s neurodevelopmental treatment. More recent publications of texts on rehabilitation for CNS problems demonstrate that the specific models used for addressing these types of problems have changed as knowledge has developed in this area. Readers are referred to more recent publications for the current approaches in this area.
Historical description of model’s development
Evident with the OP model is the influence of both the mechanistic paradigm and the beginning of the renaissance of occupation (both discussed in the introduction to this book – see Table I.1). In line with this renaissance of occupation, a change in the discourse of occupational therapy has occurred since the latter part of the twentieth century, with the term occupation becoming used pervasively. The sixth edition of Occupational Therapy: Practice Skills for Physical Dysfunction (McHugh Pendleton & Schultz-Krohn, 2006) reflects this shift towards occupation within the profession by presenting the Occupational Therapy Practice Framework (OTPF) as representing the official position of the AOTA (rather than the OP model like the previous editions). The OTPF has also been developed with the World Health Organization’s International Classification of Functioning, Disability and Health (ICF) in mind, and its relationship to the ICF is emphasized in the sixth edition. This emphasis on the ICF demonstrates the shift that has also occurred in the broader healthcare environment, in which the focus has moved away from bodily impairments alone (a biomedical approach), to activity and participation (both biopsychosocial and socioecological approaches). This movement is more aligned with the current paradigm of occupation in occupational therapy.
Occupational therapy practice framework (OTPF)
The OTPF reflects the current movement towards occupation as occupational therapy’s core concern. However, the influence of the OP model on this framework is apparent. The concepts of performance areas, performance components and context are evident within this practice framework, albeit relabelled and incorporated into more detailed and additional categories. The way that the categories of the OTPF relate to the International Classification of Function (ICF) is also made explicit in the OTPF document. The OTPF has been published in two editions − 2002 and 2008. The edition used in this chapter is from 2008 and this includes a summary of the changes made to the first edition in developing the second edition. That summary is provided on pages 665–667 of the second edition (AOTA, 2008).
The OTPF aims to make explicit both the domain and process of occupational therapy. According to McHugh Pendleton and Schultz-Krohn (2006), “the domain describes the scope of practice or answers the question: ‘What does an occupational therapist do?’ The process describes the methods of providing occupational therapy services or answers the question: ‘How does an occupational therapist provide occupational therapy services?’ (p. 10).
Domain
Client factors are “specific abilities, characteristics, or beliefs that reside within the client and may affect performance in areas of occupation” (AOTA, 2008, p. 630). As clients of occupational therapy services could be individuals, organizations or populations, this category is conceptualized as relevant to all three potential client groups. For each, the relevant values and beliefs, functions and structures are considered. For the person, values, beliefs and spirituality “influence a client’s motivation to engage in occupations and give his or her life meaning” (p. 633).
Using terminology consistent with the ICF, client factors include body functions and body structures. Quoting from a WHO publication, body functions are defined as the physiological functions of body systems (including psychological functions) and body structures refer to the anatomical parts of the body such as organs, limbs and their components. For organizations, values and beliefs might be encapsulated in vision and other value statements and codes of ethics. Functions include the processes that an organization uses for its planning, organizing and operationalizing its core functions and vision. Structures relate to the way the organization is structured including departments and their relationships, leadership and management structures, performance measures, etc. For populations, values and beliefs can include “emotional, purposive, and traditional perspectives”; functions include “economic, political, social and cultural capital” and structures “may include constituents such as those with similar genetics, sexual orientation, and health-related conditions” (AOTA, 2008, p. 634).
Activity demands “refer to the specific features of an activity that influence the type and amount of effort required to perform the activity” (AOTA, 2008, p. 634). A core skill of occupational therapists is the analysis of activities and occupations. They use this analysis to determine the capacities required for an individual to perform these activities within particular contexts. The specific constellation of demands of performing an activity or occupation provides enormous potential for altering activity demands to enable engagement in occupation. A change in one component of the activity or the context in which it is performed changes the total demands of the activity or occupation.
Performance skills have the closest relationship to performance components in the OP model. Performance skills are “the abilities clients demonstrate in the actions they perform” (AOTA, 2008, p. 639). The OTPF uses the following six interrelated categories for performance skills: motor and praxis skills, sensory-perceptual skills, emotional regulation skills, cognitive skills and communication and social skills (which have similarities to the original five categories of performance components). The OTPF distinguishes between body functions and performance skills in that body functions are capacities that “reside within the body” (p. 639) whereas performance skills are those abilities that can be demonstrated. Two of the examples that were given in the OTPF document of observable nature of performance skills are as follows: “praxis skills can be observed through client actions such as imitating, sequencing, and constructing; cognitive skills can be observed as the client demonstrates organization, time management, and safety” (p. 639). In further explicating the difference, the OTPF states “numerous body functions underlie each performance skill” (p. 639).
Performance patterns include the “habits, routines, roles, and rituals” (p. 641) that people use when engaging in activities and occupations. All four can facilitate or make difficult engagement in and performance of occupations. Habits are automatic behaviours used for engagement in occupations; routines are “established sequences of occupations or activities that provide a structure for daily life” (p. 641); roles are “sets of behaviour” (p. 641) that have social and personal expectations, can have implications for self-identity, and can shape choice and meaning of occupations; and rituals are “symbolic actions with spiritual, cultural, or social meaning that contribute to the client’s identity and reinforce the client’s values and beliefs” (p. 642). Performance patterns can develop and change over time and assist people to organize their engagement in occupations within their daily lives and over the course of their lives. The concept of performance was not a feature of the OP model, but has become embedded in occupational therapy thinking. This possibly occurred through the pervasive influence of Kielhofner’s Model of Human Occupation, presented in Chapter 6, which introduced the concept habits and routines.
Occupational therapists have always acknowledged that engagement in and performance of occupations occurs with specific places, at specific times, under specific conditions. In the OTPF, the situatedness of occupational performance is considered using the category of context and environment. It uses the term environment to refer to the physical and social environments. The physical environment refers to the natural and built environments (including the objects within them) in which people might perform occupations and the social environment “is constructed by the presence, relationships, and expectations of persons, groups, and organizations with whom the client has contact” (AOTA, 2008, p. 642).
While the term environment is used to refer to tangible aspects of the situation within which people engage in occupation, the term context is used to acknowledge the less tangible aspects of the circumstances surrounding occupational performance that can strongly influence it. These contexts can be “cultural, personal, temporal, and virtual” (AOTA, 2008, p. 642). The OTPF provides the following definitions of these four types of context, some of which are attributed to the WHO: “Cultural context includes customs, beliefs, activity patterns, behaviour standards, and expectations accepted by the society of which the client is a member. Personal context refers to demographic features of the individual such as age, gender, socioeconomic status, and educational level that are not part of a health condition. Temporal context includes stages of life, time of day or year, duration, rhythm of activity, or history. Virtual context refers to interactions in simulated, real-time or near-time situations absent of physical contact” (pp. 642 & 646). As these definitions demonstrate, the contexts surrounding occupational performance can be internal or external to the client or, in the case of cultural context, both internal and external contexts can combine – in that culture is an external context that shapes individual values and beliefs but the individual also internalizes these (to varying extents), making them part of the internal context of occupational performance.
Process
In addition to the occupational therapy domain, the OTPF also describes the “process that outlines the way in which occupational therapy practitioners operationalize their expertise to provide services to clients” (AOTA, 2008, p. 646). While the general processes that occupational therapists use, that is, assessment/evaluation, intervention and evaluating the outcomes, are also used by other professions, the OTPF document highlights that the distinctiveness of occupational therapy lies in its work “toward the end-goal of supporting health and participation in life through engagement in occupations” (pp. 646–647). Occupational therapists are also unique in that they conceptualize occupations as both methods and outcomes. Within a collaborative relationship with the client, occupational therapists plan for interventions on the basis of jointly identified and prioritized goals.
The first part of the process is assessment/evaluation. Practitioners collect sufficient appropriate information to develop an understanding of what has been, needs to be, and can be done with and for the client. The OTPF identifies this stage as consisting of both the occupational profile and analysis of occupational performance. It states, “The occupational profile includes information about the client and the client’s needs, problems, and concerns about performance in areas of occupation. The analysis of occupational performance focuses on collecting and interpreting information using assessment tools designed to observe, measure, and inquire about factors that support or hinder occupational performance.” (AOTA, 2008, p. 649.) These two components of the assessment/evaluation stage are described in detail in the OTPF document. Occupational therapists use their clinical reasoning to combine, analyze and synthesize information gained about the client’s occupational profile and occupational performance and make decisions about intervention.
Intervention is defined as “the skilled actions taken by occupational therapy practitioners in collaboration with the client to facilitate engagement in occupation related to health and participation” (AOTA, 2008, p. 652). In the OTPF, the intervention process is categorized into three steps, which are not necessarily followed in a linear sequence in practice. These are development of an intervention plan, implementation of the intervention, and its review. Each step in the intervention process is discussed in detail in the OTPF document.
The third part of the occupational therapy process relates to evaluating outcomes. The OTPF described the overall outcome of occupational therapy intervention as “supporting health and participation in life through engagement in occupation” (AOTA, 2008, p. 660). More specific outcomes are generally required to determine the degree of progress towards this more general goal that might have resulted from occupational therapy interventions. More specific outcomes might include “clients’ improved performance of occupations, perceived happiness, self-efficacy, and hopefulness about their life and abilities” (pp. 660–661). Outcomes might include information about clients’ subjective impressions of relevant goals or increments of progress that are measurable. The OTPF document proposed that “outcomes for populations may include health promotion, social justice, and access to services” (p. 661). The document outlined two steps in the outcomes process. The first was “Selecting types of outcomes and measures, including but not limited to occupational performance, adaptation, health and wellness, participation, prevention, self-advocacy, quality of life, and occupational justice” (p. 661). The second step was “Using outcomes to measure progress and adjust goals and interventions” (p. 661).

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


