Calcaneal Lengthening Osteotomy for the Treatment of Hindfoot Valgus Deformity
Vincent S. Mosca
DEFINITION
Valgus deformity of the hindfoot exists when the calcaneus is angled away from the midline of the body in relationship to the talus.
Eversion is a more specific and appropriate term for the hindfoot valgus deformity that is seen in congenital and developmental flatfoot and skewfoot deformities.
Valgus deformity of the hindfoot, which is often perhaps inappropriately referred to as pronation, is one component of eversion of the subtalar joint.
The other, and more important, components of eversion are external rotation and dorsiflexion of the calcaneus (acetabulum pedis) in relation to the plantarflexed talus.
Flatfoot is the term used to describe a weight-bearing foot shape in which the hindfoot is in valgus alignment, the midfoot sags in a plantar direction with reversal of the longitudinal arch, the forefoot is supinated in relation to the hindfoot, and the foot points in an externally rotated direction from the knee.
There is no agreement on strict clinical or radiographic criteria for defining a flatfoot. Therefore, the point beyond which a foot with a low-normal arch becomes defined as a flatfoot is unknown.
There are three recognized types of flatfoot: flexible (hypermobile) flatfoot, flexible (hypermobile) flatfoot with a short Achilles tendon, and rigid flatfoot.
Valgus deformity of the hindfoot is also seen in skewfoot, congenital oblique talus, and congenital vertical talus.
ANATOMY
Acetabulum pedis is a term that was coined by Scarpa over 200 years ago to describe and compare the subtalar joint with the hip joint because of certain similarities that exist between them. It is a cup-like structure consisting of the navicular, spring ligament, and anterior end of the calcaneus that rotates around the talus following the oblique axis of the subtalar joint.
The axis of the subtalar joint is not in any of the standard planes of motion of the body. In the transverse plane, the subtalar axis deviates about 23 degrees medial to the long axis of the foot. In the sagittal plane, the axis deviates about 41 degrees dorsal from horizontal. The summation of the angles creates an oblique axis for the subtalar joint that produces downward and inward motion during inversion and upward and outward motion during eversion.
Eversion of the acetabulum pedis results in loss of support for, and plantarflexion of, the talus. Although the calcaneus dorsiflexes “upward” in relation to the talus, it becomes plantarflexed in relation to the weight-bearing axis of the tibia. The navicular also dorsiflexes upward at the talonavicular joint as the focal point for the midfoot sag. “Outward” motion of the acetabulum pedis creates the external rotation of the rest of the foot in relation to the talus and tibia that is manifest as a positive thigh-foot angle and an out-toeing gait. Convexity of the plantar-medial border of the foot is also a manifestation of outward motion of the acetabulum pedis, reflecting the dorsolateral positioning of the navicular on the head of the talus. These altered relationships create a real, or apparent, shortening of the lateral column (or border) of the foot relative to the medial column.
A flatfoot combines valgus deformity of the hindfoot with supination deformity of the forefoot to create a low or absent longitudinal arch (FIG 1). These are rotationally opposite deformities.
The forefoot in a flatfoot is supinated in relation to the pronated/valgus hindfoot. Were it not, forefoot weight bearing would occur solely on the first metatarsal with the fifth metatarsal off the ground.
In a skewfoot, the forefoot is supinated in relation to the pronated/valgus hindfoot but pronated in relation to the midfoot. The midfoot is adducted in relation to the hindfoot.
The shapes of the bones and the laxity of the ligaments of the foot determine the height of the longitudinal arch. The muscles maintain balance, accommodate the foot to uneven terrain, protect the ligaments from unusual stresses, and propel the body forward.
The intrinsic muscles are the principal stabilizers of the foot during propulsion. Greater intrinsic muscle activity is required to stabilize the transverse tarsal and subtalar joints in a flatfooted individual than in an individual with an average height longitudinal arch.
PATHOGENESIS
Based on clinical and radiographic studies, flatfoot is ubiquitous in infants and children and is seen in over 20% of adults. The arch increases in height in most children through normal growth and development during the first decade of life. The arch decreases in height in most of those older children and adolescents who have a rigid flatfoot, a condition affecting about 2% to 5% of the population that is most often associated with a tarsal coalition.
Flexibility (hypermobility) in a flexible flatfoot refers to the motion in the subtalar joint. There is full excursion of the Achilles tendon in this class of flatfoot. It is the normal congenital foot shape seen in almost all babies and accounts for about two-thirds of the 23% of flatfooted adults. It is the normal contour of a strong and stable foot, not the cause of disability.
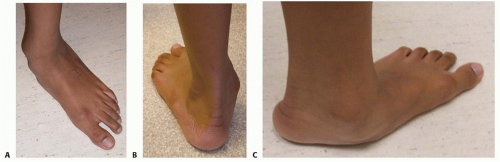
FIG 1 • Flatfoot. A. Top view shows outward rotation of the foot in relation to the lower extremity. The patella is facing forward in this image. B. Back view shows valgus alignment of the hindfoot and “too many toes” seen laterally. C. Medial view shows depression of the longitudinal arch and a convex medial border of the foot. (From Mosca VS. Calcaneal lengthening osteotomy for valgus deformity of the hindfoot. In: Tolo V, Skaggs D, eds. Master Techniques in Orthopaedic Surgery: Pediatric Orthopaedics. Philadelphia: Lippincott Williams & Wilkins, 2008:263-276.)
A flexible flatfoot with a short Achilles tendon has the same flexibility in the subtalar joint as a flexible flatfoot but has limited ankle dorsiflexion owing to contracture of the Achilles tendon. This entity accounts for about one-fourth of the 23% of flatfooted adults and often causes pain with callus formation under the head of the talus. The age or point at which the Achilles tendon contracture develops is unknown.
A contracted Achilles tendon prevents normal dorsiflexion of the talus in the ankle joint during the late midstance phase of the gait cycle. The dorsiflexion stress is shifted to the subtalar joint complex where, as a feature of eversion, the acetabulum pedis dorsiflexes in relation to the talus and also in relation to the tibia. The talus remains rigidly plantarflexed. The soft tissues under the head of the talus are subjected to excessive direct axial loading and shear stresses.
These stresses create callus formation and pain at that site.
Pain may also be experienced in the sinus tarsi region because of impingement of the beak of the calcaneus with the lateral process of the talus at the extreme range of eversion.
Rigidity in a rigid flatfoot refers to the restriction of motion in the subtalar joint. This type of flatfoot accounts for about 9% of the 23% of flatfooted adults. It is usually associated with a tarsal coalition and is, therefore, developmental rather than congenital.
The longitudinal arch gradually lowers to a flatfoot shape in these feet in late childhood, generally after the age of 8 years. This is the time at which the fibrous coalition begins undergoing metaplasia to cartilage and eventually to bone. Tarsal coalitions cause pain in less than 25% of cases. A coalition may be associated with an Achilles tendon contracture. The frequency of that association is not known.
Valgus deformity of the hindfoot is one of the segmental deformities in a congenital skewfoot, a condition for which the incidence, natural history, and even an objective definition are not known. Skewfoot also exists as an iatrogenic deformity, typically seen in a surgically treated clubfoot. Congenital and acquired skewfoot may be associated with an Achilles tendon contracture, thereby increasing its risk for creating pain in the same way that a flexible flatfoot with a short Achilles tendon may cause pain. The frequency of that association is not known.
NATURAL HISTORY
Flatfoot is a poorly defined foot shape found in most children and over 20% of adults. For most, it is an anatomic variation from average that does not cause pain or other disability.
The longitudinal arch develops spontaneously in most children during the first decade of life.
Flexible flatfoot with a short Achilles tendon often causes pain with callus formation under the head of the talus and/or pain in the sinus tarsi area.
The age or point at which the Achilles tendon contracture develops is unknown.
Rigid flatfoot causes pain in less than 25% of cases, although it causes restriction of subtalar motion in all.
Skewfoot is a poorly defined foot shape for which the natural history is not known. Review of the literature would suggest that most are, and remain, asymptomatic throughout life.
PATIENT HISTORY AND PHYSICAL FINDINGS
Children with flexible flatfoot are rarely symptomatic, although they may experience nonspecific leg or foot aches after strenuous activities or at the end of the day. Older children and adolescents with flexible flatfoot with a short Achilles tendon will often experience pain, tenderness, and callus formation under the head of the plantarflexed talus in the midfoot or in the sinus tarsi area or at both sites. About 25% of children and adolescents with a tarsal coalition report activity-related pain that may be located in the sinus tarsi area, along the medial hindfoot and/or under the head of the talus.
Commonly, parents seek consultation for their child with a painless flatfoot because of concerns regarding the appearance of the foot, the child’s uneven shoe wear, or concerns about the potential for future disability. Such concerns about future disability are based on unsubstantiated claims
by generations of health care providers that flatfoot is a deformity that requires treatment to prevent pain and disability.
Evaluation of the child’s foot should begin with a screening evaluation of the entire musculoskeletal system. The general examination includes assessment of ligament laxity, torsional and angular variations of the lower extremities, and the walking pattern. Their interrelationships are important to keep in mind during evaluation of the foot because all of these features, including the shape of the foot, change as the child grows.
Assessment of the foot begins with the recognition that a flat-foot is not a single segment deformity. It is a multisegment combination of deformities that includes a valgus/eversion deformity of the hindfoot and a supination deformity of the forefoot on the hindfoot. There is a lateral rotational deformity as well, which is a component of eversion. The axis of the subtalar joint is in an oblique plane, such that eversion creates valgus, external rotation, and dorsiflexion of the so-called acetabulum pedis around the talus.
The foot must be evaluated in weight bearing and non-weight bearing.
In weight bearing, the clinician should note the valgus alignment of the hindfoot, the depression of the longitudinal arch, and the outward rotation of the foot in relation to the sagittal plane of the tibia, which is perpendicular to the flexion-extension plane of the knee.
The flexibility of the flatfoot pertains to the mobility of the subtalar joint. A flexible flatfoot has free and supple subtalar joint motion. A rigid flatfoot has restriction of motion in that joint.
Flexibility of the subtalar joint can be assessed manually. With the hindfoot cupped in one hand and the forefoot held (for better foot control) in the other hand, the subtalar joint is inverted and everted around its oblique axis of motion using the hand that is cupping the hindfoot (FIG 2). It is important to ensure that the apparent motion is occurring in the subtalar joint and that it is not false motion through hypermobile Chopart joints.
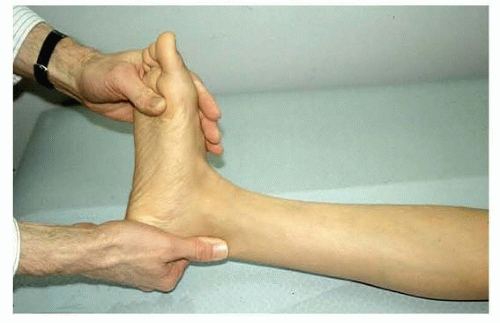
FIG 2 • Inversion and eversion of the subtalar joint is assessed by manually moving the acetabulum pedis back and forth along the axis of the subtalar joint. Forefoot supination can be appreciated when the hindfoot is inverted to neutral. While maintaining subtalar joint neutrality, the ankle is dorsiflexed with the knee first flexed and then extended to assess the excursion of the soleus and the gastrocnemius, respectively. (From Mosca VS. Flexible flatfoot and skewfoot. In: McCarthy J, Drennan J, eds. The Child’s Foot and Ankle, ed 2. Philadelphia: Lippincott Williams & Wilkins, 2010:136.)
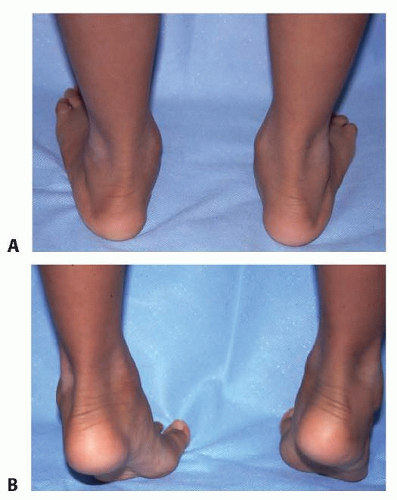
FIG 3 • A,B. With toe standing, the heel vagus converts to varus and the longitudinal arch elevates in a flexible flatfoot. (From Mosca VS. Flexible flatfoot and skewfoot. In: McCarthy J, Drennan J, eds. The Child’s Foot and Ankle, ed 2. Philadelphia: Lippincott Williams & Wilkins, 2010:136.)
Flexibility of the subtalar joint can also be assessed dynamically in weight bearing. The arch elevates and the hindfoot corrects from valgus to varus in a flexible flatfoot during toe standing (FIG 3) and with the Jack toe raise test (see Exam Table for Pediatrics: Lower Extremities). These two maneuvers take advantage of the windlass action of the plantar fascia to mobilize the subtalar joint into inversion and create a longitudinal arch.
Supination of the forefoot is revealed when the hindfoot is passively inverted to neutral alignment (see FIG 2).
Dorsiflexion of the ankle joint, as assessed by excursion of the Achilles tendon, is important yet difficult to evaluate accurately. A component of subtalar joint eversion is dorsiflexion of the calcaneus in relation to the talus. Therefore, the subtalar joint must be held inverted to the neutral position to isolate and assess the motion of the talus in the ankle joint.
The Silfverskiöld test is used to differentiate ankle joint dorsiflexion from subtalar joint dorsiflexion (see “Flexibility of the Achilles tendon and the Gastrocnemius Tendon” in Exam Table for Pediatrics: Lower Extremities).
With the subtalar joint inverted to neutral, the knee is flexed to 90 degrees. The ankle is maximally dorsiflexed without allowing the subtalar joint to evert. The degree of dorsiflexion is measured as the angle between the lateral border of the foot and the anterior shaft of the tibia. The knee is then extended while maintaining subtalar neutral, even if it creates plantar flexion of the ankle. The degree of ankle dorsiflexion is once again measured.
It is normal for the ankle to dorsiflex at least 10 degrees above neutral with the knee extended and even further with the knee flexed. The entire triceps surae (gastrocnemius and soleus) is contracted if the ankle does not dorsiflex at least 10 degrees above neutral with the knee flexed or extended. The gastrocnemius is selectively contracted if the ankle dorsiflexes at least 10 degrees above neutral with the knee flexed but not when it is extended.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Radiographs reveal the static anatomic relationships between bones. They should not be used, in and of themselves, as an indication for treatment.
Radiographs of the flatfoot are not necessary for diagnosis. They may be indicated for the assessment of pain or decreased flexibility and for surgical planning.
Weight-bearing anteroposterior (AP), lateral, medial oblique, and axial (or Harris) views are appropriate for those indications (FIG 4).
The lateral oblique (nonstandard) view is helpful for the identification of an accessory navicular that could be the cause of a painful medial prominence in the midfoot that is not the head of the talus.
An AP ankle radiograph is useful to determine whether any of the hindfoot valgus deformity is in the tibiotalar joint.
A computed tomography (CT) scan in all three planes and with three-dimensional (3-D) reconstruction is the imaging modality of choice for assessment of a rigid flatfoot, particularly when there is a high degree of suspicion for a subtalar tarsal coalition. The published criteria for operative management of a subtalar tarsal coalition are based on CT scan findings.
A bone scan can help with the assessment of atypical pain in a flatfoot.
A magnetic resonance imaging (MRI) may be indicated if these other imaging studies fail to reveal the etiology for atypical pain in a flatfoot. An MRI scan is not the imaging study of choice for evaluation of a tarsal coalition.
DIFFERENTIAL DIAGNOSIS
Flexible (hypermobile) flatfoot
Flexible (hypermobile) flatfoot with short Achilles tendon
Rigid flatfoot
Congenital oblique talus
Congenital vertical talus
Skewfoot
Pauciarticular juvenile rheumatoid arthritis affecting the subtalar joint
Peroneal spastic flatfoot

FIG 4 • Standing radiographs of a flatfoot. A. AP image demonstrates the external rotation component of eversion or valgus of the subtalar joint. B. The lateral image reveals plantarflexion of the talus, sag at the talonavicular joint, and a low calcaneal pitch. (From the private collection of Vincent Mosca, MD.)
NONOPERATIVE MANAGEMENT
Flexible flatfoot is a normal foot shape and not the cause of pain or functional disability in most individuals. Therefore, treatment must be applied only to those who have symptoms. “Prophylactic” treatment, even if nonoperative, cannot be justified, based on the literature.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



