Arthroscopy of the Wrist: Preparation and Techniques
David J. Slutsky
BACKGROUND
Since its inception, wrist arthroscopy has continued to evolve. The initial emphasis on viewing the wrist from the dorsal aspect arose from the relative lack of neurovascular structures as well as the familiarity of most surgeons with dorsal approaches to the radiocarpal joint.
Anatomic studies provided a better understanding of both the interosseous ligaments as well as carpal kinematics, which led to the development of midcarpal arthroscopy.
Innovative surgeons continue to push the envelope through the development of techniques for treating intracarpal pathology, which in turn has culminated in a plethora of new accessory portals.
ANATOMY
The standard portals for wrist arthroscopy are dorsal (FIG 1A-C). This is in part due to the relative lack of neurovascular structures on the dorsum of the wrist as well as the initial emphasis on assessing the volar wrist ligaments. The dorsal portals that allow access to the radiocarpal joint are so named in relation to the tendons of the dorsal extensor compartments.
The 1-2 portal lies between the first extensor compartment tendons, which include the extensor pollicis brevis and the abductor pollicis longus, and the second extensor compartment, which contains the extensor carpi radialis brevis (ECRB) and extensor carpi radialis longus (ECRL) (FIG 1D).
The 3-4 portal is named for the interval between the third dorsal extensor compartment, which contains the extensor pollicis longus tendon, and the fourth extensor compartment, which contains the extensor digitorum communis (EDC) tendons.
The 4-5 portal is located between the EDC and the extensor digiti minimi (EDM).
The 6R portal is located on the radial side of the extensor carpi ulnaris (ECU) tendon; the 6U portal is located on the ulnar side.
The midcarpal joint is assessed through two portals, which allows triangulation of the arthroscope and the instrumentation.
The midcarpal radial portal is located 1 cm distal to the 3-4 portal and is bounded radially by the ECRB and ulnarly by the EDC.
The midcarpal ulnar portal is similarly located 1 to 2 cm distal to the 4-5 portal and is bounded by the EDC and the EDM.
The triquetrohamate portal enters the midcarpal joint at the level of the triquetrohamate joint ulnar to the ECU tendon. The entry site is both ulnar and distal to the midcarpal ulnar
portal. Branches of the dorsal cutaneous branch of the ulnar nerve are most at risk (FIG 2A).
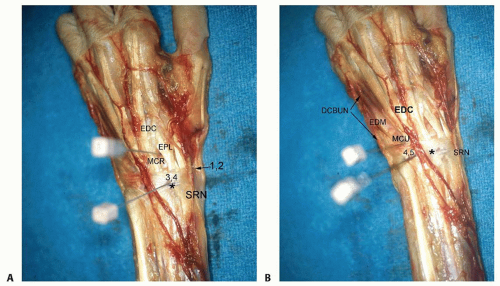
FIG 1 • Dorsal portal anatomy. A. Cadaver dissection of the dorsal aspect of a left wrist demonstrating the relative positions of the dorsoradial portals. EDC, extensor digitorum communis; EPL, extensor pollicis longus; MCR, midcarpal radial; SRN, superficial radial nerve; asterisk, tubercle of Lister. B. Relative positions of the dorsoulnar portals. EDM, extensor digiti minimi; DCBUN, dorsal cutaneous branch of the ulnar nerve. (continued)
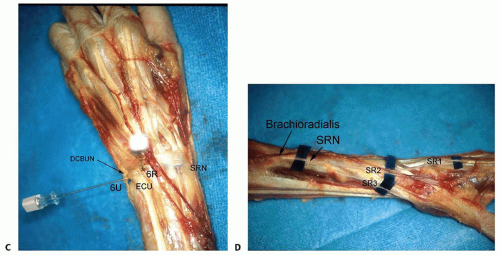
FIG 1 • (continued) C. Positions of the 6R and 6U portals. ECU, extensor carpi ulnaris. D. Branches of the superficial radial nerve (SRN). SR1, minor dorsal branch; SR2, major dorsal branch; SR3, major palmar branch. (From Slutsky DJ. Wrist arthroscopy portals. In: Slutsky DJ, Nagle DJ, eds. Techniques in Hand and Wrist Arthroscopy. Philadelphia: Elsevier, 2007.)
The dorsal radioulnar joint portal lies between the ECU and the EDM tendons. Transverse branches of the dorsal cutaneous branch of the ulnar nerve are the only sensory nerves in proximity to the dorsal radioulnar portal at a mean of 17.5 mm distally (range 10 to 20 mm) (FIG 2B,C).
There are two volar portals that can be used to access the radiocarpal joint.
The volar radial portal is accessed through the floor of the flexor carpi radialis (FCR) tendon sheath at the level of the proximal wrist crease.4,7,9
Anatomic studies revealed that there is a safe zone free of any neurovascular structures equal to the width of the FCR tendon plus at least 3 mm in all directions.
The volar aspect of the midcarpal joint can be accessed through the volar radial midcarpal portal. The same skin incision is used but the capsular entry point is about 1 cm distal.
The volar ulnar portal is located underneath the ulnar border of the flexor tendons at the level of the proximal wrist crease.6
The volar aspect of the distal radioulnar joint (DRUJ) can be accessed through the volar distal radioulnar portal using the same skin incision, but the capsular entry point for the volar distal radioulnar portal lies 5 mm to 1 cm proximal to the ulnocarpal entry point (FIG 2D,E).
NONOPERATIVE MANAGEMENT
In general, wrist arthroscopy is indicated as a diagnostic technique in any patient with persistent wrist pain that has not responded to an appropriate trial of conservative measures:
Nonsteroidal anti-inflammatories and activity modification
Cortisone injection
Wrist arthroscopy is used as an adjuvant procedure for the treatment of acute fractures of the distal radius or scaphoid or for staging degenerative disorders involving the carpus.
Indications
The indications for the use of the standard dorsal portals are intertwined with the indications for wrist arthroscopy and depend largely on the condition that is being treated.
A typical arthroscopic examination of the wrist will include variable combinations of the 3-4 portal, the 4-5 portal, and the 6R and 6U portals.
The 3-4 and 4-5 portals are the main viewing portals for the radial aspect of the radiocarpal joint and for instrumentation.
The 4-5 and 6R portals are used to access the ulnocarpal joint.
The 6U portal is typically used for outflow.
The volar radial portal is indicated for the evaluation of the dorsal radiocarpal ligament (DRCL) and the palmar portion of the scapholunate interosseous ligament (SLIL). The volar radial portal also facilitates arthroscopic reduction of intraarticular fractures of the distal radius fractures by providing a clear view of the dorsal rim fragments.
The volar ulnar portal is indicated for visualizing and débriding palmar tears of the lunotriquetral ligament. It also aids in the repair or débridement of dorsally located triangular fibrocartilage (TFC) tears because the proximity of the 4-5 and 6R portals makes triangulation of the instruments difficult.
Midcarpal arthroscopy through the dorsal midcarpal portals is essential in making the diagnoses of scapholunate and lunotriquetral instability.
The grading scale reported by Geissler and colleagues2 provides a means for staging the degree of instability and provides an algorithm for treatment.
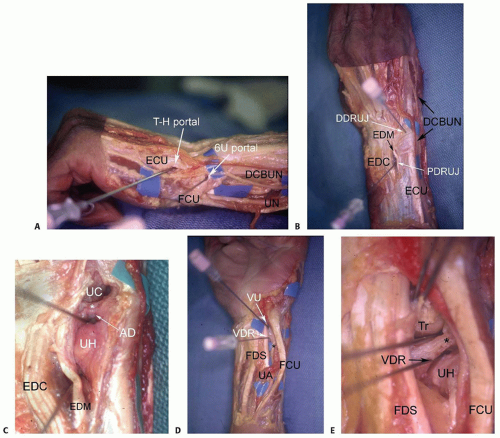
FIG 2 • A. Ulnar aspect of a left wrist demonstrating the relative positions of the triquetrohamate (T-H) portal and the 6U portal. ECU, extensor carpi ulnaris; FCU, flexor carpi ulnaris; DCBUN, dorsal cutaneous branch of the ulnar nerve; UN, ulnar nerve. B,C. Dorsal DRUJ portal anatomy. B. Relative position of the proximal DRUJ (PDRUJ) and distal DRUJ (DDRUJ) portals. C. Close-up with the dorsal capsule removed demonstrating the position of the needles in relation to the dorsal radioulnar ligament (asterisk). UC, ulnocarpal joint; AD, articular disc; UH, ulnar head; EDC, extensor digitorum communis; EDM, extensor digiti minimi. D,E. Volar DRUJ portals. D. Volar aspect of a left wrist demonstrating the relative positions of the volar ulnar (VU) and volar DRUJ (VDR) portals in relation to the ulnar nerve (asterisk) and ulnar artery (UA). FDS, flexor digitorum sublimis; FCU, flexor carpi ulnaris. E. Close-up view after the volar capsule is removed showing position of needles in relation to the volar radioulnar ligament (asterisk). Tr, triquetrum. (From Slutsky DJ. Wrist arthroscopy portals. In: Slutsky DJ, Nagle DJ, eds. Techniques in Hand and Wrist Arthroscopy. Philadelphia: Elsevier, 2007.)
Midcarpal arthroscopy is likewise employed for the assessment and treatment of chondral lesions of the proximal hamate.
The triquetrohamate joint can also be accessed through another special-use midcarpal portal.1
The volar radial midcarpal portal is occasionally used as an accessory portal for visualizing the palmar aspects of the capitate and hamate in cases of avascular necrosis or osteochondral injury.
This portal facilitates visualization of the palmar aspect of the capitohamate interosseous ligament, which is important in minimizing translational motion and has an essential role in providing stability to the transverse carpal arch.
The volar DRUJ portal is useful for assessing the deep foveal attachment of the triangular fibrocartilage complex (TFCC), which would normally require an open capsulotomy.
It may be employed if the suspicion of a peripheral TFCC detachment remains despite the absence of any visible TFCC tears through the standard ulnocarpal portals.
The dorsal DRUJ portal may be used in concert with the volar DRUJ portal to more completely assess the status of the articular cartilage of the ulnar head and sigmoid notch as well as for instrumentation.
The number of conditions amenable to arthroscopic treatment continues to grow. Many arthroscopic procedures are now common, whereas others await clinical validation. Table 1 provides a list of the more standard procedures.
Table 1 Arthroscopic Wrist Procedures | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
|
Contraindications
Contraindications to the use of dorsal or volar portals would include marked swelling, which distorts the topographic anatomy; large capsular tears, which might lead to extravasation of irrigation fluid; neurovascular compromise; bleeding disorders; or infection.
Unfamiliarity with the regional anatomy is a relative contraindication.
SURGICAL MANAGEMENT
It is useful to have a systematic approach to viewing the wrist.
The structures that should be visualized as a part of a standard examination include the radius articular surface; the proximal scaphoid, lunate, and triquetrum; the SLIL and lunotriquetral interosseous ligament (LTIL), both palmar and dorsal; the radioscaphocapitate ligament; the long radiolunate ligament; the radioscapholunate ligament; the ulnolunate ligament; the ulnotriquetral ligament; the articular disc; and the radial and peripheral TFCC attachments.
Many procedures can be done without fluid, which minimizes the amount of swelling and fluid extravasation. Intermittent irrigation with a 10-mL syringe attached to the inflow portal of the arthroscope followed by suction with the full radius resector can help clear the field.
The volar radial portal is used in patients with radial-sided and dorsal wrist pain to visualize the palmar SLIL and the DRCL.
In patients with ulnar-sided wrist pain, the volar ulnar portal is used to assess the palmar LTIL and dorsal radioulnar ligament, the region of the ECU subsheath, and the radial TFCC attachment.
The scope is then inserted in the 3-4 portal followed by various combinations of the 4-5 portal and 6R portal. The 6U portal is mostly used for outflow, but it may be used for instrumentation when débriding palmar LTIL tears.
Midcarpal arthroscopy is then performed to probe the SLIL and LTIL joint spaces for instability, the capitohamate interosseous ligament, and to look for chondral lesions on the proximal capitate and hamate and loose bodies.
The special-use portals such as the dorsal and volar DRUJ portals and the 1-2 portal are used as needed.
Preoperative Planning
A 2.7-mm, 30-degree angled scope along with a camera attachment is used.
Table 2 describes the typical field of view as seen through a 2.7-mm arthroscope under ideal conditions.1,3Related posts:
 Open Reduction and Internal Fixation of Pediatric T-Condylar Fractures
Elbow Replacement for Acute Trauma
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures
Open Reduction and Internal Fixation of Pediatric T-Condylar Fractures
Elbow Replacement for Acute Trauma
Open Reduction and Internal Fixation of Ulnar Styloid, Head, and Metadiaphyseal Fractures
Fragment-Specific Fixation of Distal Radius Fractures
Vascularized Bone Grafting and Capitate Shortening Osteotomy for Treatment of Kienböck Disease
Operative Treatment of Metacarpal Fractures

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


