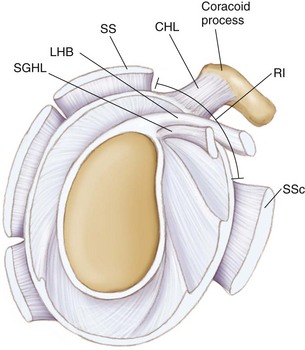
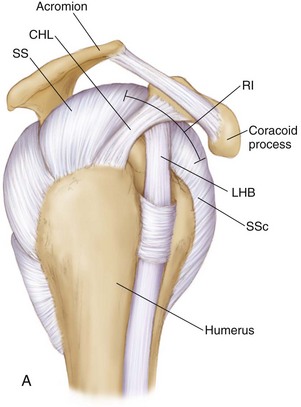
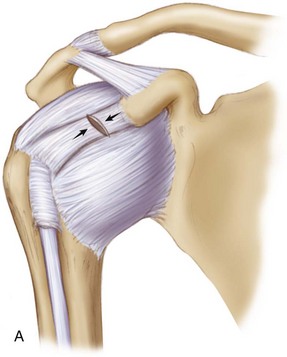
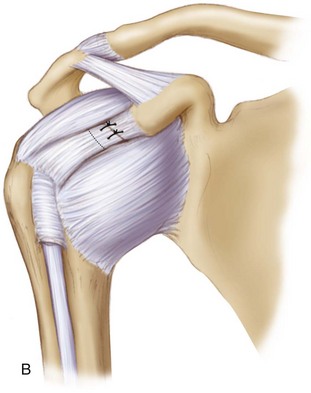
Chapter 6 • The rotator interval (RI) is a triangular space of the anterosuperior shoulder between the supraspinatus and subscapularis tendons. The function of the RI in maintaining overall shoulder stability remains under debate, but surgical closure of the RI has been advocated in specific cases of shoulder instability. In the past, RI closure was commonly performed via open surgical techniques; however, recent all-arthroscopic techniques for RI closure have been described. The purpose of this chapter is to describe the arthroscopic treatment for RI closure. • The components of the RI include the coracohumeral ligament (CHL), the superior glenohumeral ligament (SGHL), the long head of the biceps (LHB) tendon, and a thin layer of joint capsule. • The RI is a triangular space between the supraspinatus (SS) and subscapularis (SSc). • The RI shape changes with internal and external rotation of the glenohumeral (GH) joint. • A competent RI contributes to inferior shoulder stability via the CHL and an intact shoulder capsule (maintains negative intraarticular pressure). • A sulcus sign that persists in external rotation (ER) is an indicator of RI insufficiency (of the CHL). • Hyper-ER of the arm at the side (more than 90 degrees) also suggests incompetent anterior stabilization structures (possibly the RI). • An open RI closure imbricates the CHL better than an arthroscopic closure; thus an open RI closure does not perform the same biomechanically as an arthroscopic RI closure, as both techniques generally repair different tissues in a different vector of closure. • Volumetric reduction of the GH joint capsule may be achieved with adequate RI closure. • Adequate visualization from posterior portal. • Arthroscopic closure medially and laterally (two separate stitches) in robust tissue of SGHL and middle glenohumeral ligament (MGHL). • Penetrator device or suture passer may be used to accomplish repair—generally a 1-cm imbrication of the capsular tissues. • Some advocate SS to SSc closure to obtain more robust tissue closure. • Tie the sutures over the capsule blindly through a cannula that is pulled out just anterior to the capsule before tying. • Imbrication of the CHL medially to laterally is difficult to achieve with arthroscopic methods. Clinical and Surgical Pitfalls • Closing the RI in neutral will result in ER losses, especially at the side; close the RI in 30 to 45 degrees of ER to avoid loss of ER postoperatively. • Avoid suturing the LHB tendon so as not to imbricate the biceps. • For inadequate shift of tissue, use two stitches—one medially and one laterally based—to obtain an adequate shift. • Performing RI closure when not indicated will not improve stability and possibly will lead to large losses in motion. The rotator interval (RI) is a triangular space of the anterosuperior shoulder between the supraspinatus (SS) and subscapularis (SSc) tendons, containing both the coracohumeral ligament (CHL) and the superior glenohumeral ligament (SGHL) (Figs. 6-1 and 6-2). Although injuries to the RI capsule have been associated with increased glenohumeral translation and subsequent instability,1,2 its contribution to overall shoulder stability remains under debate. Several reports have suggested that RI capsular structures contribute to stability by resisting inferior and posterior glenohumeral translation3–6 and/or maintaining negative intraarticular pressure,7 whereas others have shown that surgical imbrication of the RI augments surgical correction of multidirectional and posterior instability.3,4,6,8–12 Previously, RI closure was commonly performed via open surgical techniques; however, recent all-arthroscopic techniques for RI closure have been described.13,14 The debate regarding RI closure is centered around the “circle concept” of the shoulder,15 which states that if the humerus is posteriorly subluxed, there must be an opposite and obligate injury to the anterior superior structures of the glenohumeral joint (the RI). However, several studies have refuted the circle concept theory,16 indicating no injury to the RI after posterior dislocation. In addition, the premise of an open RI closure is not the same concept as an arthroscopic RI closure.3,14,17 As described by Harryman,3 open RI closure consistently imbricates the CHL from medial to lateral, which adequately restores inferior and posterior stability of the shoulder; however, this occurs at the expense of significant (30- to 40-degree) losses of external rotation (ER) at the side (Fig. 6-3). All-arthroscopic techniques have evolved to address the RI; however, the arthroscopic closure is fundamentally different from the open closure in direction of closure (arthroscopic: superior to inferior; open: medial to lateral and/or superior to inferior), in addition to differences in tissue imbricated (arthroscopic: RI capsule, SGHL to middle glenohumeral ligament [MGHL]; open: CHL or SS to SSc). Based on biomechanical evidence,12,14,17–19 there are certain indications for an arthroscopic RI closure, including certain cases of anterior instability (in the setting of hyperlaxity) and revision anterior instability (to increase the bumper effect anteriorly), multidirectional instability with laxity and sulcus sign, and possible posterior or anterior instability in the setting of hyperlaxity. The purposes of this chapter are to review the operative indications and surgical technique for arthroscopic RI capsule closure in the setting of glenohumeral instability. Figure 6-3 The coracohumeral ligament (CHL) is sectioned (A) and then imbricated by 1 cm (B), as was demonstrated by Harryman3 in an open rotator interval closure that shortened the CHL to improve inferior and posterior stability of the shoulder. This technique resulted in significant (30- to 45-degree) losses of external rotation at the side. • Original mechanism of injury (traumatic versus insidious onset) • Current symptoms (may point to alternative diagnosis) • Pain (e.g., rest pain vs. night pain) • Inability to use arm above head • Previous nonsurgical and surgical treatment of the shoulder • Activity level of the patient • Posttreatment goals; allows the surgeon to address patient expectations and to ensure that these are aligned with treatment options and outcomes • Sulcus sign—downward traction of the arm causes inferior subluxation of the humeral head that does not resolve with ER of the shoulder (Fig. 6-4).
Arthroscopic Rotator Interval Capsule Closure*†
Preoperative Considerations
Physical Examination
Related posts:
 Open Repair of Posterior Shoulder Instability
Open Repair of Posterior Shoulder Instability
 Osteochondral Autograft for Cartilage Lesions of the Knee
Osteochondral Autograft for Cartilage Lesions of the Knee
 Arthroscopic Rotator Cuff Repair: Double-Row Techniques
Arthroscopic Rotator Cuff Repair: Double-Row Techniques
 Surgical Treatment of Posterolateral Instability of the Elbow
Surgical Treatment of Posterolateral Instability of the Elbow
 Primary Repair of Osteochondritis Dissecans in the Knee
Primary Repair of Osteochondritis Dissecans in the Knee
 Arthroscopic Meniscus Repair: All-Inside Technique
Arthroscopic Meniscus Repair: All-Inside Technique
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Arthroscopic Rotator Interval Capsule Closure
 Video
Video