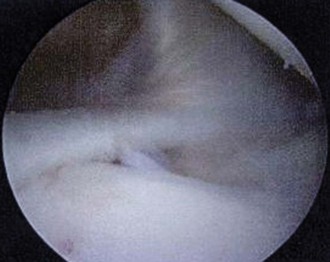
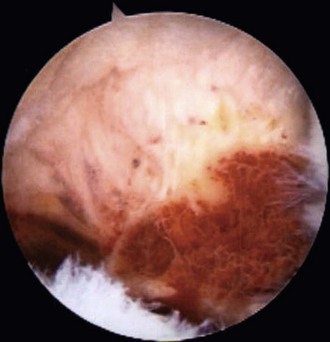
Chapter 8 • The superior labrum has a wide variety of normal anatomy, and the understanding of what really constitutes a pathologic process is critical to know when repair is indicated. • Synovitis of the shoulder may be commonly encountered, but an understanding of areas in which it may extend extra-articularly, as in the axillary and rotator interval, is useful. • Extra-articular fractures may extend into the glenoid surface, necessitating arthroscopic monitoring of the reduction to ensure adequate joint restoration. • Instability lesions are often complex, with multiple areas of damage. A complete and thorough inspection of the entire capsulolabral complex, including both humeral and glenoid attachments, should be considered essential in evaluating and correcting these injuries. • Avoid making holes in the tendons of the rotator cuff. • Complete the diagnostic arthroscopy before establishing accessory portals. • Use K-wires placed via fluoroscopy into the mobile fragments before beginning arthroscopic fracture management. • Repair instability by beginning inferiorly and medially, progressing to the lateral inferior, and then moving front to back while slowly progressing toward the superior aspect of the shoulder. Radiographs are usually normal except in synovial osteochondromatosis, in which multiple loose bodies are noted (Fig. 8-1). Magnetic resonance imaging (MRI) is helpful for osteochondritis dissecans lesions, synovial cysts (Fig. 8-2), and chondrolysis. Avulsions of a Buford complex, PVNS, and articular cartilage fractures will not show up on most radiographic tests. Glenohumeral avulsions are visualized by arthrography, and the coracoid fracture is best noted on computed tomographic scans. Avulsion of the Buford complex attachment is the most difficult to differentiate from normal variants. It is thought that the presence of the Buford complex has an incidence of 1.5% to 6.5%,1,2 but the frequency with which it is avulsed is unknown. Chondromalacia of the glenoid and fraying of the undersurface of the labrum and outer surface of the glenoid isolated to that area alone and not farther inferior on the glenoid are key findings (Fig. 8-3). In all joints, PVNS has an incidence of approximately 1.8 cases per 1 million people.3 Eighty percent of cases occur in the knee. PVNS is rare in the shoulder and has the characteristic appearance seen in other joints.3 However, it is not readily resected because it penetrates through the lining of the joint and expands outward into the surrounding structures (Fig. 8-4). Especially in inferior lesions, the synovial growth may envelope the axillary nerve, necessitating its dissection either through open surgery or by arthroscopic identification of the nerve and protection of it.
Arthroscopic Management of Rare Intra-articular Lesions of the Shoulder
Preoperative Considerations
Imaging
Surgical Technique
Examination: Diagnostic Arthroscopy and Specific Steps per Rare Entity
1 Avulsion of the Buford Complex Attachment
2 Pigmented Villonodular Synovitis
Related posts:
 Open Repair of Posterior Shoulder Instability
Open Repair of Posterior Shoulder Instability
 Osteochondral Autograft for Cartilage Lesions of the Knee
Osteochondral Autograft for Cartilage Lesions of the Knee
 Arthroscopic Rotator Cuff Repair: Double-Row Techniques
Arthroscopic Rotator Cuff Repair: Double-Row Techniques
 Surgical Treatment of Posterolateral Instability of the Elbow
Surgical Treatment of Posterolateral Instability of the Elbow
 Primary Repair of Osteochondritis Dissecans in the Knee
Primary Repair of Osteochondritis Dissecans in the Knee
 Arthroscopic Meniscus Repair: All-Inside Technique
Arthroscopic Meniscus Repair: All-Inside Technique
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


Arthroscopic Management of Rare Intra-articular Lesions of the Shoulder
 Video
Video