CHAPTER 25 Arthroscopic Management of Pediatric Hip Disease
Surgical technique
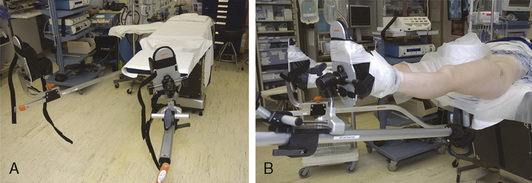
Hip arthroscopy can be performed with the patient in the supine or lateral decubitus position. Both positions allow for adequate visualization and positioning, and the one that is used is based on surgeon preference. We perform hip arthroscopy with the patient in the supine position, and it is generally performed as an outpatient procedure for the pediatric population. General anesthesia is used with muscle relaxation, although supplementation with regional anesthesia may be used, depending on the anesthesia available and patient preference. A standard fracture table or a specialized hip-scope table is used with a traction device and a large padded perineal post (Figure 25-1). The affected leg is prepped and draped along with a C-arm (Figure 25-2). The nonoperated side is placed in approximately 30 degrees of abduction, and firm traction is applied to that side so that the patient remains firmly against the perineal post. The operated leg is placed in neutral abduction to maintain a constant relationship between the topographic landmarks and the joint. A slight 10 degrees of flexion is used to relax the capsule; however, excessive flexion and traction can place tension on the sciatic nerve. Maximal internal rotation is used to make the femoral neck parallel with the floor. Traction is applied to achieve joint distraction between 5 mm and 10 mm, and this is confirmed by fluoroscopy; this will typically demonstrate the “vacuum sign” when viewed with the use of fluoroscopy. In general, approximately 50 lb to 75 lb of force is needed to distract a joint. The goals are to use the minimal force necessary to achieve distraction and to keep traction times as brief as possible (in general, less than 2 hours is considered optimal).

Portals
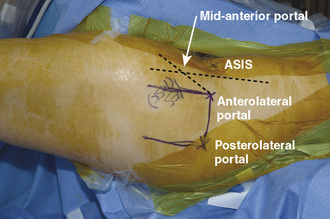
Two to three operating portals are typically used. The anterolateral and posterolateral portals are placed at the superior margin of the greater trochanter at the anterior and posterior borders (Figure 25-3). The mid-anterior portal is made by first drawing a sagittal line from the anterosuperior iliac spine and another line at the anterolateral portal; a sagittal line is then drawn equidistant to these two lines. The entry point for the mid-anterior portal is approximately 45 degrees from the anterolateral portal on the middle sagittal line. With careful attention paid to these landmarks, the portals can be safely made away from neurovascular structures. The lateral femoral cutaneous nerve typically lies just medial to the anterosuperior iliac spine; the femoral nerve and artery are even more medial.
< div class='tao-gold-member'>
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


