 FIGURE 4.1 Panner disease. AP radiograph of the left elbow demonstrating fragmentation and lucency of the capitellum (circle) near the chondral surface. |
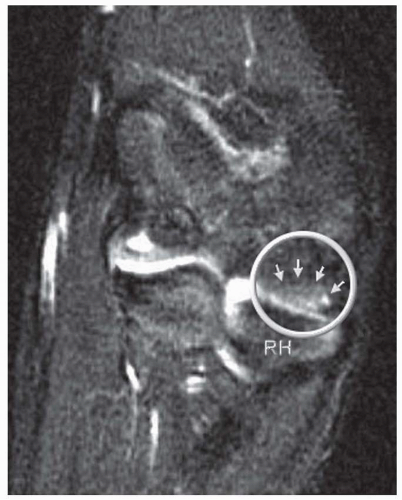 FIGURE 4.2 Panner disease, as seen on T2-weighted MRI. Circle surrounds Panner lesion, demarcated by small arrows, opposite radial head (RH). Notice the more typical finding of edema adjacent to the capitellar chondral surface, rather than deeper in the subchondral bone as in OCD. |
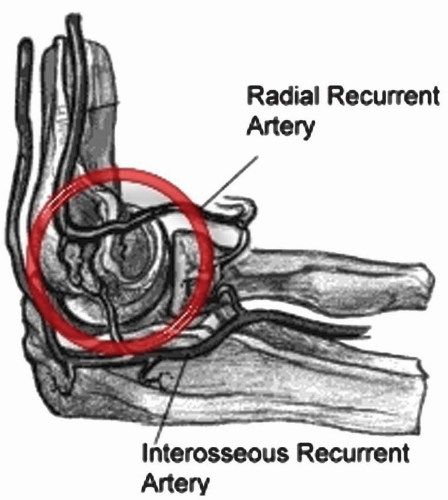 FIGURE 4.3 Capitellar blood supply. In the young adult population (under age 20), the radial recurrent and interosseous recurrent arteries give off branches that course from posterior to anterior and supply the capitellum (inside red circle). This end-artery blood supply makes the capitellum susceptible to an avascular insult. |
 FIGURE 4.4 Radiocapitellar compression test. Pain in lateral elbow when the extended arm is pronated and supinated. |
partially detached piece from subchondral bone (Fig. 4.6). Peiss et al. (19). felt that fragment enhancement (seen in Fig. 4.7B) (as opposed to the perifragment enhancement seen in Fig. 4.6) denotes viability and may be a reasonable indication for nonoperative treatment. They also suggested that enhancement of the fragment-subchondral bone interface is caused by vascular granulation tissue, indicating instability and requiring operative intervention. Of note, it is critically important to distinguish “pseudolesions,” appearing on the posteroinferior
junction of the articular and nonarticular portions of the capitellum, from OCD which almost always presents on the anterolateral aspect. In addition, whether or not the capitellar physis is open or closed should be noted.
 FIGURE 4.5 AP radiograph at 45 degrees flexion. OCD lesion (circle) is seen more clearly with elbow flexed to 45 degrees. |
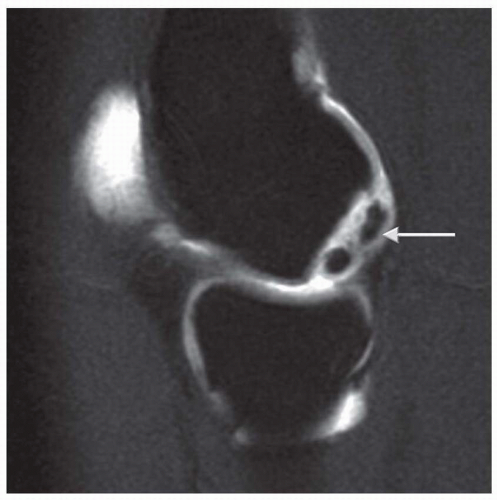 FIGURE 4.6 MR arthrogram showing contrast surrounding unstable OCD fragment (arrow). |
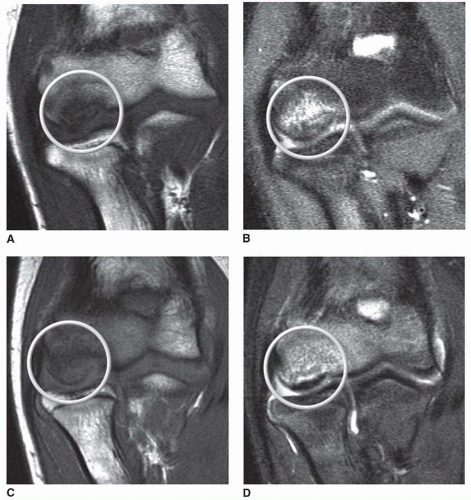 FIGURE 4.7 Stage 1 OCD lesion progress. Stable, intact, nondisplaced fragment (circles) with abnormal signal on coronal slices in (A) T1 and (B) T2 sequences. After 6 months of conservative management (C) T1 and (D) T2 sequences show reconstitution of subchondral bone in area the lesion. The patient was symptom free at the 6-month follow-up. |
TABLE 4.1 Classification and Treatment of Capitellar Osteochondritis Dissecans Lesions | |||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| |||||||||||||||||||||||||||||||||||||||||||||||||
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


