CHAPTER 18 Arthroscopic Iliopsoas Release and Lengthening
Surgical technique
Iliopsoas Release at the Lesser Trochanter
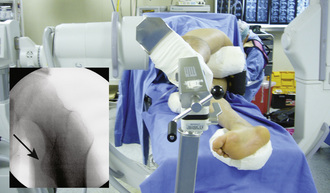
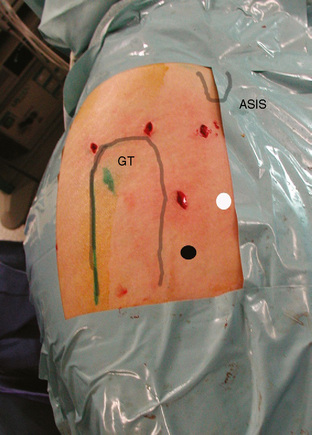
After hip arthroscopy of the central and peripheral compartments is complete, the instruments are taken out of the joint. The hip is positioned in 20 degrees of flexion and external rotation to expose the lesser trochanter at the image intensifier (Figure 18-1). A spinal needle is introduced through an accessory portal (i.e., the superior accessory portal) that is established about 2 cm distal to a horizontal line directed anteriorly from the tip of the greater trochanter and 2 cm anterior to the anterior femur (Figure 18-2). The needle is directed toward the lesser trochanter and navigated by the image intensifier (Figure 18-3). Orientation in the coronal plane is provided by the image intensifier. Orientation in the sagittal plane is provided by palpating the anterior aspect of the femur until the needle is positioned on the lesser trochanter; this will position the needle inside of the iliopsoas bursa. After the spinal needle has been successfully positioned in the iliopsoas bursa, the stylus is removed, and a flexible guidewire (Nitinol) is introduced. The needle is removed, and a cannulated switching stick is passed into the iliopsoas bursa over the flexible guidewire. A 4.5-mm, double-valve, rotatable arthroscopic cannula is passed over the switching stick, which is then removed, and then a 4-mm, 30-degree arthroscope is introduced. The fluid pump is started, and the iliopsoas tendon is identified. A second accessory portal 3 cm to 4 cm distal to the first one is established (i.e., the inferior accessory portal). A spinal needle is triangulated toward the tip of the arthroscope inside of the iliopsoas bursa. The image intensifier can be used to assist with the navigation of the needle. The tip of the needle is identified endoscopically inside of the iliopsoas bursa, and a working portal is established with the use of a flexible guidewire, a cannulated switching stick with a dilator, and a slotted cannula (Hip Access System, Smith and Nephew, Andover, MA). A shaver is introduced through the slotted cannula, which is then removed. The shaver is used to resect synovial tissue from the iliopsoas bursa and to dissect the iliopsoas tendon. The slotted cannula is reinserted with the use of the shaver as a guide. The shaver is removed, and a radiofrequency hook probe is inserted; the slotted cannula is removed, and the radiofrequency probe is used to release the iliopsoas tendon close to its insertion on the lesser trochanter (Figures 18-4 and 18-5). The image intensifier can be used to verify the position of the radiofrequency hook probe before the release of the iliopsoas tendon.
< div class='tao-gold-member'>
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


