Ankle Arthrodesis
A Literature Review
Keywords
• Ankle arthrodesis • Ankle arthritis • Ankle fixation • Arthrodesis
Introduction
Ankle arthrodesis has become the mainstay surgical procedure for end-stage ankle arthritis.1–3 There are a vast array of surgical approaches to this procedure. The end goal of any ankle arthrodesis procedure should be a well-aligned ankle joint with the foot at a 90° angle to the leg. A well-positioned ankle fusion can be very successful in alleviating pain, correcting the deformity, and restoring a functional limb.
Indications
Preoperative planning of an ankle fusion can be extensive. Before making the decision of fusing the ankle joint, the surgeon must evaluate the integrity of the surrounding joints, in particular the subtalar joint. The surgeon must take into consideration the amount of compensation that will come from the midtarsal joints, tarsal-metatarsal joints, and the subtalar joints. Wu and colleagues4 found that sagittal plane motion for the forefoot and transverse plane motion of the rearfoot increased after an ankle joint fusion. It is recommended that preoperative radiographs include foot, ankle, and leg films. This is especially important if considering intramedullary rod fixation, as deformity of the tibia can make insertion of the nail challenging.
Contraindications
Although fusion of the ankle joint may relieve pain and symptomatology for the right patient, contraindications do exist. Patients unable to be cleared for surgery secondary to medical issues, such as uncontrolled diabetes or poor nutritional status, should not be taken to surgery. Peripheral vascular status must be evaluated and the patient should be educated on the detrimental effects of tobacco use in relation to healing potential. When considering ankle fusion with internal fixation, bone infection is also a contraindication, and other forms of fixation may be warranted, specifically external fixation.5
Surgical approach
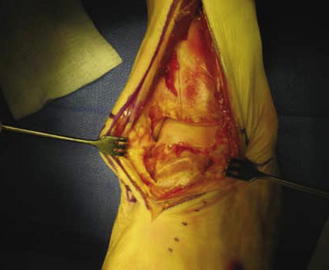
Midline anterior approach allows great exposure to the anterior ankle joint. This incision is made just lateral to the border of the tibialis anterior tendon (Fig. 1). Care must be taken to avoid damaging the medial dorsal cutaneous nerve. Through this incision, the ankle joint is exposed between the tibialis anterior tendon and the extensor hallus longus tendon. The disadvantage of this incision is that it lacks exposure to the posterior ankle joint and the malleoli. The surgeon should consider this approach when the talus has been displaced medial or lateral under the tibia in the frontal plane.
A lateral approach, otherwise known as the transfibular approach, is a common technique used today. It involves a hockey stick incision over the lateral aspect of the distal one-third of the fibula, courses the sinus tarsi, and ends at the base of the fourth metatarsal. This approach should be considered when the foot is translated forward after an old pilon fracture or when the lateral malleolus must be removed. When using this approach, the surgeon must do a fibular osteotomy to access the ankle joint (Figs. 2 and 3). This approach is excellent to visualize the lateral ankle joint (Fig. 4). After completion of the ankle joint fusion, the surgeon may use the fibula as an onlay graft; however, it is not recommended to anatomically repair the fibula. Mahan and colleagues6 report an increased incidence of delayed or nonunion when the fibula was anatomically repaired.



Winson and colleagues7 reviewed 105 arthroscopic ankle arthrodeses. The investigators used anteromedial and anterolateral portals to access the ankle joint. Articular cartilage was removed with a soft tissue debrider and curettes. The lateral gutter was cleared enough to allow compression of the joint, and articular surfaces of the medial malleolus were removed. The investigators used a burr to remove bone until punctate bleeding was visualized in cancellous bone. Anterior tibial osteophytes were removed with the scope. Once the joint was fully prepared and cleaned, 2 percutaneous 6.5-mm screws were placed medially from the tibia to the talus. Penetration into the subtalar joint was avoided. The average time to union was 12 weeks. Nonunion occurred in 9 patients. Seven of the nonunions were successfully fused using an open arthrodesis technique. The investigators modified their postoperative protocol following a significant number of nonunions within the first 8 cases. Immobilizing the operative site for a longer period (12 weeks) postoperatively was initiated, and a decrease in the number of nonunions was seen. The investigators stated that a decreased time to union occurs in arthroscopic arthrodesis because periosteal stripping is not necessary and local circulation to the bone remains intact. Nineteen percent of these patients required removal of screws because of prominence.
Miller and Myerson8 described the mini-arthrotomy approach using 2, 1.5-cm incisions anterior medially and anterior laterally. The anterior medial incision was made just medial to the anterior tibial tendon at the level of the joint and the anterior lateral incision was made lateral to the peroneus tertius tendon at the level of the joint. With the anterior lateral incision, care must be taken to avoid the superficial peroneal nerve. A small lamina spreader was placed in the portal not being used to open the joint and allow debridement. This process was then switched to allow debridement of the other side of the joint. This approach allows limited access to the posterior aspect of the joint, but, as previously described, the limited posterior aspect of the joint that cannot be reached is inconsequential for the arthrodesis. Debridement technique is surgeon choice, but burring should be limited because of possible necrosis of the subchondral bone.
Multiple techniques have been described in the literature for preparing the ankle joint for fusion. The simplest technique is removal of cartilage from the tibia and the talus by joint resection or curettage (Figs. 5 and 6). Other techniques have been described, such as anterior bone grafting to facilitate fusion, joint resection with combined malleolar osteotomy, subtotal or incomplete resection of the articular cartilage, and compression arthrodesis. No matter what joint preparation the surgeon chooses, Glissan principles for successful fusion should be used. Glissan described 4 requirements for successful fusion, which include complete removal of all cartilage, accurate and close fitting or fusion surfaces, optimal position, and maintenance of bone apposition in an undisturbed fashion until fusion is achieved.9,10 Shortening of the limb can be seen; however, if joint surfaces are prepared carefully, less than 1 cm of shortening is seen.


Optimal position of an ankle joint fusion is 0 to 5° of rearfoot valgus, 5 to 10° of external rotation (transverse plane should be in line with the normal Malleolar axis), and foot in a 90° position to the leg. Literature states that up to 5° of plantarflexion of the foot on the leg can be tolerated. Position of the fusion is the key to a successful procedure. Malalignment in the sagittal plane with ankle joint in equinus can lead to genu recurvatum. Coronal plane position is equally important with unsatisfactory results seen when the heel is in varus, leading to painful callosities to the lateral forefoot11 and increased hindfoot symptoms.12,13 It is important to consider equinus when positioning the foot. If a marked equinus is present during physical examination, an Achilles tendon or gastrocnemius lengthening may need to be performed to allow the foot to be permanently fixed at a 90° angle to the lower leg. Zwipp and colleagues14–22 recommend performing a percutaneous lengthening of the Achilles tendon in patients with an equinus greater than 10°.
When fusing the ankle joint, it is important to keep in mind the 4 following principles for a successful fusion: (1) good alignment of the fusion with the rearfoot aligned to the leg and the forefoot to the rearfoot; (2) apposition of broad, flat, vascularized bony surfaces; (3) stable and rigid internal or external fixation; and (4) compression across the arthrodesis site.23
Fixation approach
The 2-screw fixation technique, as described by Ogilvie-Harris and colleagues,24 places 1 screw from the medial malleolus into the talus and 1 screw from the lateral malleolus into the talus. A cadaver study comparing 2-screw and 3-screw fixation was performed by Ogilvie-Harris and colleagues.24 The investigators determined that the 3-screw construct gave increased compression when compared with the 2-screw construct. The 2-screw construct is not commonly used today, as other techniques have proven to be more stable and provide more compression at the arthrodesis site (Figs. 7–9).







Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


