7. Applied stretches to common muscle groups
Soft tissue stretching is an intricate part of sports activity, and is generally a necessity to achieve the desired ROM and musculofascial health each sport requires. Since there are many methods of stretching (see Chapter 6) it is also important to utilize the techniques correctly when applying them to different sports scenarios. Research has demonstrated that static stretching can reduce muscular power output and speed when used immediately prior to athletic activity (Bazett-Jones et al. 2008; Cè 2008, Chaouachi 2008, Herda 2008, Herman 2008, Holt 2008, McHugh 2008, Mirca 2008, Samuel 2008, Torres et al, 2008 and La Torre, 2010), especially when the muscle is in a shortened position and if performed after active warm-up (CèCè 2008 and McHugh 2008). Static stretching of the upper body seems to generate fewer negative effects in regard to strength (Torres et al. 2008), and it has been suggested that athletes may perform upper-body static stretching without power reduction, provided sufficient time is allowed before the event (Torres et al. 2008). Some studies on static stretching indicate negative effects on speed, endurance, and power performance in muscles of the lower body when carried out close to athletic activity (Samuel 2008 and Wilson J.M., 2010.), while it is also suggested that acute static stretching does not negatively affect high-intensity aerobic exercise performance (Samogin Lopes et al. 2010). On the other hand, dynamic stretching techniques have been demonstrated to produce beneficial effects like increased jump power and sprint performance, especially when combined with elements of resistance (Jaggers J.R., 2008. and Needham, 2009). Dynamic warm-ups have been shown to produce increased strength, sustained power, muscular endurance, anaerobic capacity, and agility among wrestlers (Herman & Smith 2008), and consequently today it is generally recommended to utilize dynamic warm-up routines, including dynamic stretches, prior to imminent athletic performance (Herman 2008, Needham, 2009, Sekir U, 2010., Fletcher and Monte-Colombo, 2010 and Torres et al, 2008). It is even suggested that static stretching should be utilized only during post-practice or competition (Bazett-Jones et al. 2008), but also indicated that static stretching utilized in combination with active movements like sprint training reduces some of the negative effects commonly associated with static stretching and sports performance (Chaouachi et al. 2008). Additionally, there is also the opinion that musculotendinous stiffness may contribute to optimizing power output in explosive movements, and furthermore potentially guard an athlete against sports injuries (Wilson & Flanagan 2008).
Focal stretching
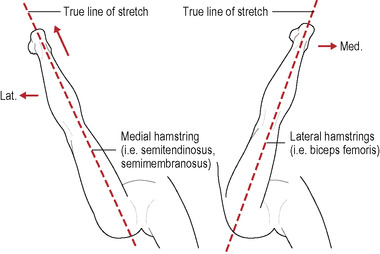
To ensure both full control and effect in treated tissues during the stretch, the lever (often an arm, leg, or neck) to which the muscles are attached is moved in specific angles. For example, to focus the stretch on the lateral aspect of a muscle or body part, the lever is moved medially before the stretch commences. An imaginary line can be drawn through the lever to the muscle (or conversely, from the intended section of the muscle out through the lever), taking the general stretch direction into consideration (Fig. 7.1), to see exactly where the stretch effect will end up. In this way, specific fiber sections of a muscle can be selected for a very precise and effective stretch. This method works well for flexion, extension, abduction, adduction, etc., but not as well for rotational movements, where the lever is better viewed as a “spool” around which the tendon is “rolled up.”
 |
| Figure 7.1 |
Therapeutic stretching is always three-dimensional, and it is important the sports therapist thinks in a functional manner. Therapeutic stretching in sports treatment is commonly performed from many different positions, and it is customary for the therapist to improvise and adapt to the situation at hand. By thinking three-dimensionally, it is easier to assess the “true lines of stretch.” The stretch movements are commonly the opposite of the treated muscle’s actions, where each movement is performed in sections toward its respective end point. This enables complete control of the stretch, and presents the possibility of focusing on specific restricted movements in a general movement pattern. The therapist must, however, be aware that the actions of a muscle can change depending on the position of the lever. One example of this is the piriformis muscle, which changes action from lateral rotation to medial rotation when the hip joint is flexed more than approximately 60–90 degrees. Another example is the supraspinatus muscle, which performs medial rotation instead of the normal lateral rotation when the glenohumeral joint is positioned in strong adduction. This again stresses the importance of thinking functionally and “three-dimensionally” during therapeutic muscle stretching.
Another important aspect of therapeutic stretching is the concept of an initial manual fixation of origin, insertion, muscle belly, and/or fascia. By fixating the tissue prior to the stretch, the effect is focalized, and joint movement reduced. Fixating can also minimize the stress on an inflamed tendon while the rest of the muscle can still be stretched effectively. The tissue is often fixated obliquely into the muscle and away from the direction of stretch. The muscle can also be pushed into a “C-shape” during the stretch to focalize the effect. A pressure applied after the stretch is initiated tends to have an effect in more superficial layers, whereas if it is applied just prior to the stretch, more deeply situated fibers are affected. Specific massage strokes and soft tissue techniques may also be applied to a stretch to increase its effectiveness. This is described in more detail in Chapter 14.
A tensed muscle will activate the reciprocal inhibition reflex (see Chapter 6) and thereby “weaken” its antagonists. It may therefore be advantageous to precede the stretch with one or more isometric contractions of the antagonist to reactivate the weakened muscle. This may also cause some relaxation in the treated target muscle even before the actual stretch commences. This procedure may generate a more “balanced” joint after the stretch is completed.
The use of accessories
Even though it is desirable for the sports therapist to develop adequate skill to stretch athletes without additional equipment in order to minimize equipment dependency, certain situations may require the use of props. Stretching straps (Fig. 7.2) enable areas of the body to be fixated to facilitate specific and effective stretching. Blocks and wedges may be used to help keep heavier body parts elevated during a stretch, and/or assist a smaller therapist to work more effectively on large and strong athletes.
 |
| Figure 7.2 |
Methods
All stretch methods previously mentioned in Chapter 6 can be used on any stretched muscle or muscle group (Figs 7.3; 7.4). The decision of which method to employ depends on personal preference, desired effect, and the specific need in the athletic scenario.
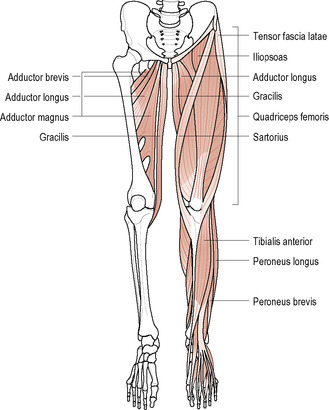 |
| Figure 7.3 |
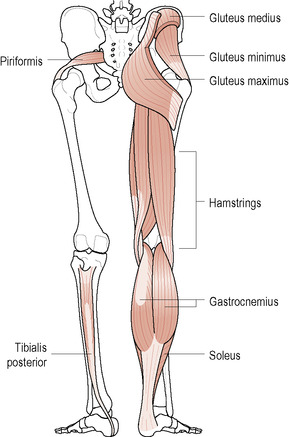 |
| Figure 7.4 |
Common stretches for the lower body
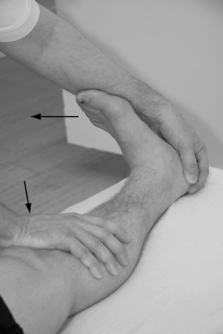
Therapeutic stretch of tibialis anterior muscle
The athlete lies supine. The therapist dorsal flexes the athlete’s foot to relax the muscle, and uses the palm heel to fixate the muscle by pushing into the muscle with an additional cranial direction of 45 degrees (Fig. 7.5). The muscle is stretched as the athlete’s foot is pushed into plantar flexion and eversion with simultaneous increased fixation force.

Therapeutic stretch of tibialis posterior muscle
1. The athlete lies prone with the treated leg in 90-degree flexion at the knee joint.
2. The therapist gently grasps the athlete’s heel, and presses the foot into dorsal flexion with the forearm (Fig. 7.6). The pressure is more on the lateral aspect of the ball of the foot, which generates a needed eversion.

Therapeutic stretch of peroneal muscle group
1. The athlete lies prone with the stretched leg in 90-degree flexion at the knee joint.
2. The therapist fixates the muscle proximally with one hands thumb, grasps the ball of the foot with the other hand, and presses the foot into dorsal flexion (Fig. 7.7). The pressure is on the medial aspect of the ball of the foot to generate an additional inversion of the foot.
 |
| Figure 7.7 |
Therapeutic stretch of triceps surae muscle group
1. The athlete lies supine. The therapist grasps the heel and presses the foot into dorsal flexion with the forearm. The pressure is on the ball of the sole of the foot.
General stretch of the hamstring muscle group (Fig. 7.9)
Previous injuries should be noted prior to stretching the hamstrings to possibly include potential cautionary measurements, and/or prestretch fibrotic treatment techniques.
 |
 |
 |
 |
| Figure 7.9 Stretch of the hamstring muscle groupA General stretch of the hamstring muscle group B Semitendinosus/semimembranosus C Biceps femoris D Modified hamstring stretch |
1. The athlete lies supine. The therapist places the athlete’s leg on one shoulder. The athlete’s hip joint is pushed into further flexion while the two hands, placed immediately superior to the knee joint, pull to simultaneously extend the knee joint. The therapist pushes the leg anterior with an additional 45-degree superior angle to keep a certain level of traction, which also prevents the knee from bending during the stretch (see Fig. 7.9A).
2. To stretch the medial hamstrings more specifically, the leg is either abducted until the true line of stretch overlaps the muscles, or laterally rotated, which also will distance origin and insertion (see Fig. 7.9B).
3. The biceps femoris is stretched by adducting the leg, or medially rotating the straightened leg as the hip joint is moved into increased flexion (see Fig. 7.9C).
4. For more flexible athletes, the therapist may place the athlete’s heel in the web between the thumb and index finger. With the therapist’s body lined up (see Fig. 7.9D) the athlete’s leg is pushed into further hip flexion, traction, and knee extension.
Stretch of quadriceps femoris (Fig. 7.10)
1. The athlete lies prone. The therapist flexes the athlete’s knee joint, and the hip and pelvis are fixated to the table by the therapist’s forearm or hand (see Fig. 7.10A). The fixation is on the inferior aspect of the sacral area. The athlete’s foot is pushed toward the gluteus maximus muscle.





2. To focalize the stretch to the vastus lateralis muscle, the athlete’s foot is pushed toward the opposite gluteal area (see Fig. 7.10B). The stretch can also be accentuated if the therapist simultaneously fixates the vastus lateralis muscle by pushing it into a “C-shape.”
3. The athlete’s foot is pushed laterally to the hip joint to focalize the stretch to vastus medialis. One hand stabilizes the pelvis (see Fig. 7.10C), or can also push the muscle into a “C-shape” prior to the stretch phase.
Note that stretches 2 and 3 are applied only on healthy knee joints. The initial fixation is most important here to minimize the lateral and medial movement.
4. The therapist places one knee under the athlete’s thigh, just superior to the patella, to generate extension in the athlete’s hip joint. The hip and pelvis are fixated and leveled to the table by the therapist’s forearm, and in addition the hand of the same arm pulls the opposite hip toward the therapist (see Fig. 7.10D). The fixation is on the inferior aspect of the sacral area to avoid further extension of the lumbar spine. The therapist slowly generates flexion in the athlete’s knee joint to stretch the muscle to the end point.
5. The athlete lies prone on the table with one foot on the floor. The therapist fixates the athlete’s heel with one foot (see Fig. 7.10E). One hand stabilizes the athlete’s pelvis. The stretched leg is aligned straight to focalize the stretch to the rectus femoris muscle, and the knee is flexed until the end point of the muscle is reached.
Stretch of the adductor group
1. The athlete lies supine with one leg slightly abducted and the lower leg hanging off the treatment table. The therapist locks the athlete’s leg with one thigh (Fig. 7.11) and leans gently away from the table to create traction in the hip joint. The muscles are stretched as the leg is pushed into further abduction.

2. Adductor magnus stretch. The posterior aspect of the adductor magnus muscle is stretched by adding a slight flexion in the hip joint.
Stretch of the gracilis muscle
The athlete lies supine with the treated leg straight and slightly abducted. The therapist locks the athlete’s leg with one thigh (Fig. 7.12) and leans gently away from the table to create traction in the hip joint. The toes should point straight up to affect the target muscle and minimize hamstring involvement. The muscle is stretched as the leg is pushed into further abduction.
 |
| Figure 7.12 |
Stretch of the sartorius muscle
The athlete lies supine with one leg slightly abducted and hanging off the treatment table. The nontreated leg is either hanging over the opposite side of the table, or is fixated with a stretch strap. The therapist locks the athlete’s treated leg by grasping around the thigh and pressing against the shoulder, and leans gently away from the table to create traction in the hip joint. The therapist additionally performs an abduction, extension, and medial rotation of the hip joint to stretch the muscle (Fig. 7.13).
< div class='tao-gold-member'>
Only gold members can continue reading. Log In or Register to continue
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


