Anatomic Repair of Lateral Ankle Instability
Gregory C. Berlet
B. Collier Watson
Christopher F. Hyer
Terrence M. Philbin
DEFINITION
Ankle sprains are the most common athletic-associated injury: They represent up to 40% of all sports-related injuries. The incidence of this inversion type of ankle sprain is around 10,000 people per day.
Literature has cited that about 50% of patients with ankle sprains have some long-term sequelae of their injury. Many of these people develop ankle instability.
Ankle instability can be divided into two categories, functional and mechanical.
Functional instability refers to the subjective feeling of the ankle giving way during activity.
Mechanical instability is the term used when patients show excessive ankle motion, beyond the normal physiologic barriers.
ANATOMY
The lateral ankle is supported by both dynamic and static structures (FIG 1).
Static structures include the bony architecture of the joints and the ligaments. This bony configuration contributes about 30% of the stability, whereas the remaining 70% of stability comes from the soft tissues.
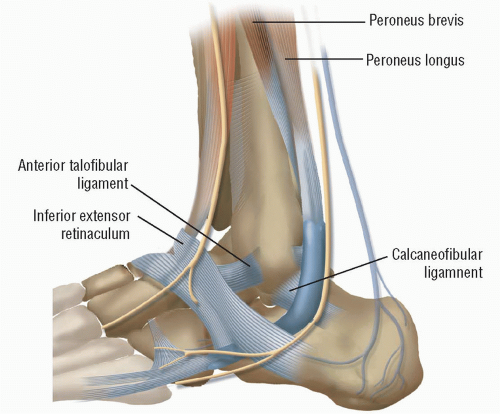
FIG 1 • The relative positions of the sural nerve, the lateral branch of the superficial peroneal nerve, and the inferior extensor retinaculum.
The dynamic structures that aid in the stability of the ankle include the peroneus longus and peroneus brevis tendons. These tendons run posterior to the fibula in the peroneal groove. They are kept in this groove by the superior peroneal retinaculum.
Once the tendons pass the distal tip of the fibula, they alter their course and run along the lateral border of the calcaneus, under the inferior peroneal retinaculum, with the peroneus brevis inserting on the base of the fifth metatarsal and the peroneus longus making another turn at the cuboid tunnel and inserting on the first metatarsal.
These two tendons act as the primary evertors of the ankle and also participate in plantarflexion of the ankle. As a result of their course and function, they work in a dynamic fashion to provide stability to the ankle and subtalar joints.
In addition to the bony configuration of the joint, the static restraints for the lateral aspect of the ankle include the anterior talofibular ligament (ATFL), the calcaneofibular ligament (CFL), and the posterior talofibular ligament (PTFL).
The ATFL is the most frequently injured ligament and the weakest of the three ligaments. It is flat and broad and originates from the anterior border of the lateral malleolus and continues anteromedially to insert on the talar body, anterior to the articular surface.
The CFL originates just inferior to the ATFL on the anterior border of the lateral malleolus and runs deep to the peroneal tendons and in a posterior, inferior, and medial direction to insert on the posterior aspect of the lateral calcaneus.
The PTFL is the strongest of this lateral ankle complex and is rarely injured. It originates from the posterior aspect of the fibula, deep to the peroneals, and inserts on the lateral tubercle of the talus, laterally to the flexor hallucis longus groove.
With the ankle plantarflexed, the ATFL is taut and becomes vertical, acting as a collateral ligament. In dorsiflexion, the same is true for the CFL.
The ATFL has been shown to be the primary restraint to inversion in the ankle.
PATHOGENESIS
Injury to the lateral ligamentous complex of the ankle is common. These inversion ankle injuries often result in attenuation or rupture to one or more of these ligaments.
With the loss of these static restraints, the ankle becomes mechanically unstable, moving past the normal physiologic restraints for the ankle joint (FIG 2).
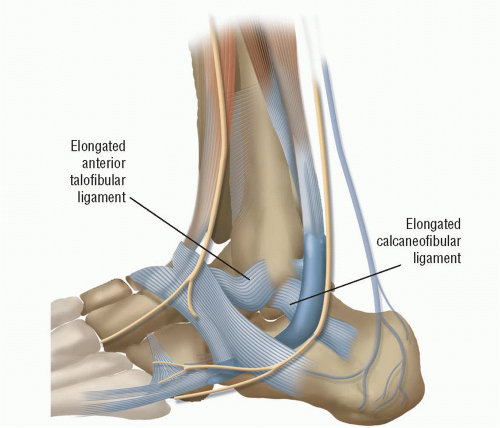 FIG 2 • Position of the elongated ATFL and CFL. |
NATURAL HISTORY
Once injury to the lateral stabilizers of the ankle has occurred, the patient should undergo immobilization followed by progressive rehabilitation.
If this approach fails, it is usually related to peroneal weakness, proprioceptive defects, subtalar instability, and mechanical or functional instability.
Chronic ankle instability can lead to repetitive inversion injuries, with the potential for fracture, osteochondral lesions of the talus, peroneal tendon injury and dislocation, and significant posttraumatic arthritis.
PATIENT HISTORY AND PHYSICAL FINDINGS
Patients with chronic lateral ankle instability will describe an inversion injury in the past. As a result, they will report that they have problems with consistent repetitive ankle sprains, a feeling of looseness in the ankle with or without pain.
The physician should inquire whether the patient is experiencing pain between intervals of repetitive injury. This would point toward the possibility of a secondary problem from instability (ie, osteochondritis dissecans, impingement lesion, synovitis).
The examination for chronic lateral ankle instability includes evaluation of the joint above (knee) and below (subtalar). Assessment should include overall alignment, range of motion, point of maximal tenderness, anterior drawer testing, evaluation of the peroneal tendons for pathology, ankle proprioception, and evaluation for associated injuries.
Alignment should be evaluated for both the overall lower limb and the hindfoot. Patients with hindfoot varus alignment are predisposed to ankle inversion injuries and instability. The alignment is assessed in both the seated and standing positions. The flexibility of the hindfoot should be checked.
Patients whose malalignment cannot be corrected with orthoses should have the alignment addressed at the time of operative ligament repair.
Tibiotalar as well as subtalar joint motion should be evaluated. Ankle motion has been described as ranging from 13 to 33 degrees of dorsiflexion and 23 to 56 degrees of plantarflexion.
The variability is dependent on the operator and the mode of measurement.
Accepted values for functional range of motion are 10 degrees of dorsiflexion and 25 degrees of plantarflexion.
Range-of-motion testing can always be compared to the uninjured side for comparison.
Subtalar motion occurs about an oblique axis running from the medial side of the talar neck to the posterolateral wall of the calcaneus. Total motion for inversion and eversion is an arc of 20 degrees, but this is extremely difficult to assess accurately. The predominance of this motion is inversion.
The anterior drawer test is designed to test the competency of the ATFL.
The test is performed with the patient seated and the knee flexed to 90 degrees. The tibia is stabilized with one hand while the ankle rests in relaxed plantarflexion. The contralateral hand is used to draw the talus anteriorly.
If the medial restraints are intact, then the movement has a rotatory component. Increased talar displacement when compared to the contralateral limb indicates a positive test. In addition, excessive motion alone can signify incompetency of the ATFL.
Most resources cite an absolute value of 10 mm for a positive test. A firm end point should also be noted when testing for ATFL competency.
Proper examination of the ankle for chronic instability includes the evaluation of the peroneal tendons. These tendons can easily be injured at the time of the varus stress that tears the ATFL as well as with the recurrent instability that follows.
Evaluation for swelling in the retrofibular space is performed.
Simple palpation of the tendons (for tenderness) and strength testing are mandatory.
Peroneal weakness mandates a search for peroneal pathology.
The peroneal compression test can be helpful as well. The patient should be examined in a dynamic way to elicit peroneal subluxation or dislocation if it is present.
Proprioception testing is an essential part of evaluating chronic ankle instability. Defects in proprioception following ankle sprains are well documented in the literature.
The modified Romberg test or stabilimetry is the best way to assess proprioception. A modified Romberg test is performed by having the patient stand first on the uninjured limb, with eyes open and then closed; this is then repeated on the injured side.
The difference in balance is related to the proprioception pathways of each limb.
The limitation of this test is that, to be accurate, there should be a full range of motion of the ankle and the subtalar joint and no pain with full weight bearing.
The advantage of the Romberg test is that it requires no special equipment.
Stabilimetry measures postural equilibrium and correlates with functional instability, but data generated on total sway in the vertical and horizontal planes require a force plate and computer analysis.
Finally, the examiner must rule out other possibilities on the differential diagnosis and determine whether there is more than one source of pathology.
Point tenderness in the area of the fifth metatarsal base, the anterior calcaneal process, and the lateral talar process could represent fracture.
Full evaluation of the ankle joint for loose bodies, osteochondritis dissecans lesions, and impingement lesions should be performed.
IMAGING AND OTHER DIAGNOSTIC STUDIES
The use of imaging in the patient with the symptoms of ankle instability should begin with three plain radiographic views of the ankle.
These films should be evaluated for fractures of the fifth metatarsal, lateral talar process and anterior process of the calcaneus, as well as fractures to the malleoli.
In addition, the examiner should be looking for exostoses of the tibia and talus, osteochondral lesions of the talus, and tarsal coalitions.
Stress radiography can be used to evaluate anterior talar translation and talar tilt. A standardized apparatus would improve reliability and consistency in this measure. The use of the contralateral limb as a control should be included when using this measure for a surgical indication.
Further studies to evaluate the lateral aspect of the ankle include the use of magnetic resonance imaging (MRI). MRI can delineate peroneal tendon pathology as well as provide needed information about osteochondral lesions of the talus (FIG 3).
DIFFERENTIAL DIAGNOSIS
Bone
Anterior process of calcaneus fracture
Lateral posterior talar process fracture
Lateral malleolus fracture
Base of fifth metatarsal fracture
Tibiotalar bony impingement
Tarsal coalition
Cartilage
Osteochondral lesions of talus or tibia
Subtalar cartilage flap tear
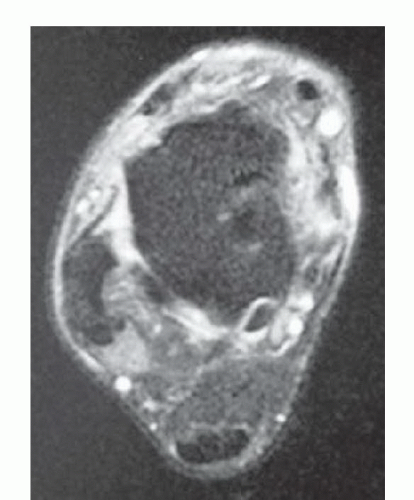
FIG 3 • MRI with torn ATFL.
Ligamentous
Functional lateral ankle instability
Mechanical lateral ankle instability
Subtalar instability
Syndesmosis injury
Neural
Neurapraxia of the superficial peroneal nerve
Neurapraxia of the sural nerve, reflex sympathetic dystrophy
Tendons
Peroneus brevis tendon tear
Peroneus longus tendon tear
Painful os peroneum syndrome
Peroneal subluxation or dislocation
Soft tissue
Anterolateral ankle impingement lesion
Sinus tarsi syndrome
NONOPERATIVE MANAGEMENT
Nonsurgical treatment of lateral ankle instability begins with restricted activity and physical therapy.
Physical therapy should focus on stretching, proprioception, and peroneal tendon strengthening.
In addition, braces and shoe wear modification can be used. The use of a lateral heel wedge, a flared sole, and a reinforced counter can assist patients with instability.
External stabilization of the ankle joint with taping or wrap dressings can provide some stabilization. Studies have shown superior initial resistance to inversion with taping, but taping has been shown to lose 50% of this initial effectiveness after 10 minutes of exercise.
As a result, the use of over-the-counter reusable braces is recommended for nonoperative stabilization of the ankle joint. A University of California Berkeley orthosis, an ankle-foot orthosis (AFO), or a hinged AFO may also be used to help patients avoid surgery.
In more sedentary patients, these modalities may provide adequate treatment, but for most athletes, they are unacceptable for long-term care.
SURGICAL MANAGEMENT
Surgery for chronic ankle instability is indicated following a trial of failed nonoperative management.
Patients with persistent, symptomatic mechanical instability will benefit from ligament reconstruction. This is often the case for athletes as well as patients who cannot tolerate bracing on a long-term basis.
Relative contraindications for surgery include pain with no instability, peripheral vascular disease, peripheral neuropathy, and inability to comply with postoperative restrictions.
Many procedures have been described for the management of ankle instability. They can be subdivided into anatomic and nonanatomic reconstruction techniques.
The authors’ choice for lateral ankle ligament reconstruction is influenced and based on the patient’s body habitus, activity pattern, and physical demands.Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree



