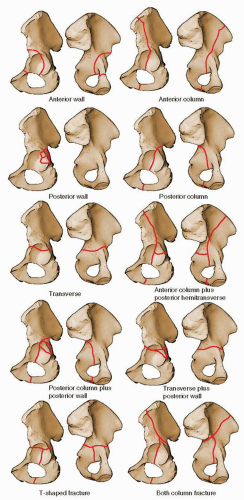
 FIGURE 41.1 Letournel acetabular fracture classification. (From Moed BR, Reilly M. Fractures of the acetabulum. In: Rockwood and Green’s fractures in adults. 7th ed. Philadelphia, PA: Lippincott Williams & Wilkins; 2009:1475, Figure 45.14.) |
TABLE 41.1 Acetabular Fracture Classification | ||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| ||||||||||||||||||||||||||
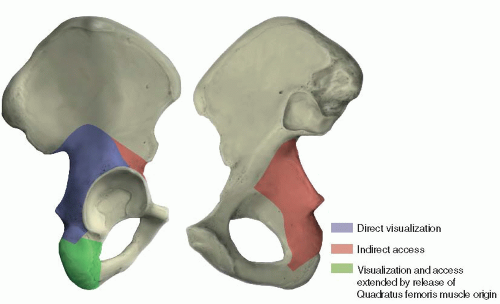 FIGURE 41.2 Access provided by the Kocher-Langenbeck approach. |
 FIGURE 41.3 A,B. Examples of available instruments for acetabular fracture reduction. Special instruments that permit intrapelvic and anterior column access (A). Other useful reduction clamps, from left to right: large reduction forceps with points; pelvic reduction clamp; large pelvic reduction forceps with pointed ball tips; straight ball spike; Farabeuf reduction forceps; and serrated reduction forceps (B). |
preclude use of the Kocher-Langenbeck approach. More recently, a percutaneous method has been reported in a small number of patients, using a plastic brush to débride the injured fatty tissue, which is then washed from the wound with pulsed lavage (3). A medium closed-suction drain is placed within the lesion and removed when drainage is <30 mL over 24 hours. Fracture fixation is deferred until at least 24 hours after drain removal.
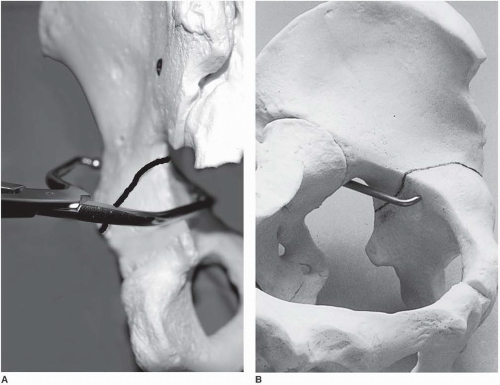 FIGURE 41.4 A,B. Example of clamp application for fracture reduction with a bone model. (A: Copyright Berton R. Moed, MD, St. Louis, MO, and Mark S. Vrahas, MD, Boston, MA. Permission granted.) |
planning (Fig. 41.7). The eventual universal availability of high-quality three-dimensional CT reconstructions may eliminate much of the mystery associated with the radiographic interpretation of acetabulum fractures (Fig. 41.8). However, except for the AP hip x-ray, which in most cases provides the same information as the AP pelvis examination, the plain and two-dimensional CT radiographic studies continue to be indispensable and should be viewed concurrently to make the definitive fracture diagnosis (2).
 FIGURE 41.5 Initial AP pelvis x-ray of a 20-year-old man involved in a motor vehicle accident. There is a transverse fracture of the left acetabulum with a vertical fracture line through the ischium, suggestive of an atypical T-shaped pattern. A double density just lateral to the femoral head suggests a displaced intra-articular or wall-fracture component. The right hip is subluxed, but not dislocated, and there is widening of the right sacroiliac joint. |
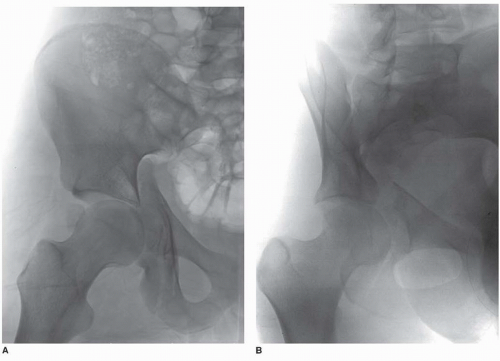 FIGURE 41.6 A-C. Subsequent AP and 45-degree oblique hip x-rays visualize the atypical T-shaped acetabular fracture more completely. However, the additional fracture components are not well delineated. |
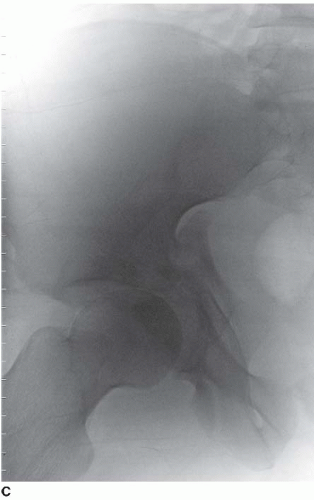 FIGURE 41.6 (Continued) |
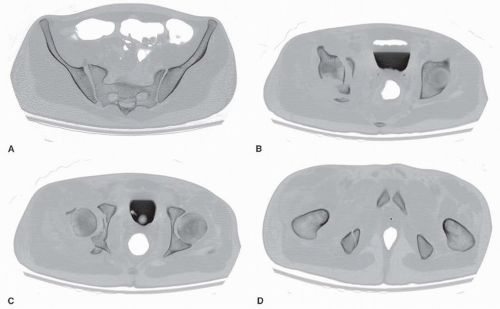 FIGURE 41.7 Selected two-dimensional CT sections. In addition to the previously noted findings consistent with an atypical T-type fracture, a posterior wall fracture fragment, and two osteochondral-free fragments (one intra-articular and one displaced anterior to the femoral head) are evident. |
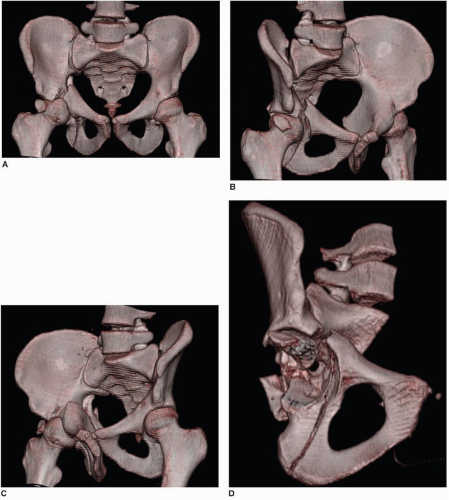 FIGURE 41.8 A-D. Three-dimensional CT constructs formed as AP and 45-degree oblique views (A-C) and created using the volume-rendering technique show very clearly the fracture as deduced by evaluation of the plain x-rays and two-dimensional CT. An excellent overall appreciation of the fracture pattern is provided. A three-dimensional construct subtracting the femur and oriented obliquely into the hip joint (D) shows the fracture comminution; however, there is some loss of definition. |
TABLE 41.2 Indications for Emergency Acetabular Fracture Fixation | ||||||||
|---|---|---|---|---|---|---|---|---|
|
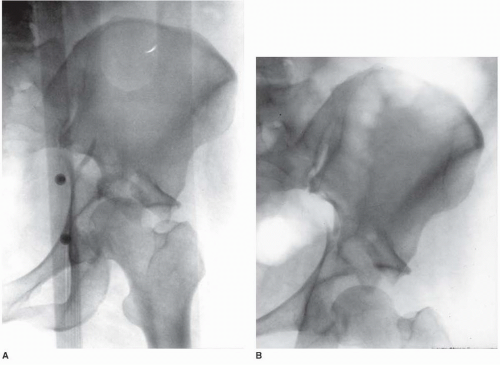 FIGURE 41.9 AP hip radiographs before and after the application of traction. A. Without traction, the femoral head is medially subluxed, rubbing against the sharp corner of the superior acetabular fracture surface in this displaced transtectal fracture. B. The hip joint is distracted with the application of traction pulling the articular cartilage of the femoral head a safe distance away from the acetabular fracture surface. |
 FIGURE 41.10 Lateral position for surgery on the right hip. The patient is supported on a beanbag on a radiolucent operating room table. The down leg is padded, and an axillary roll and head supports are in position. For this patient with an ipsilateral ankle fracture, the right leg is splinted and padded. |
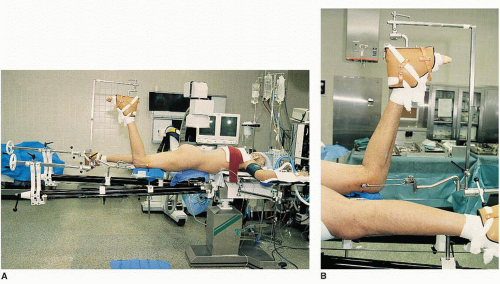 FIGURE 41.11 Patient in the prone position for surgery on the right hip (A) with a detailed view of the affected limb and femoral pin position (B). |
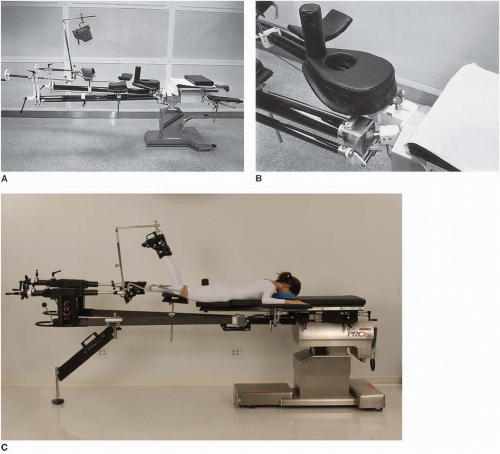 FIGURE 41.12 The Judet fracture table. A small pad can be used to elevate the patient’s head (A). A detailed view (B) shows the padded perineal post and the padded support with perineal cutout for male patients. The separation between the chest and padded perineal support serves to reduce abdominal pressure without requiring additional padding or chest rolls. The currently available PROfx Fracture Table version (C) manufactured by Mizuho OSI (Figure courtesy of Mizuho OSI, Union City, CA. Permission granted.) |
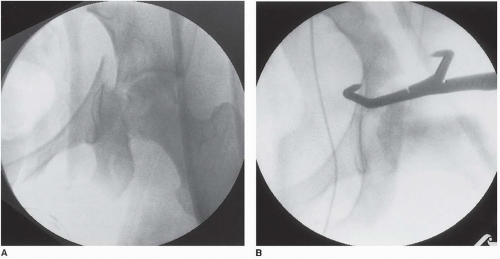 FIGURE 41.13 Intraoperative fluoroscopic views of a transverse with an associated posterior-wall fracture before (A) and after (B) the transverse fracture component was reduced by using a pointed reduction forceps. |
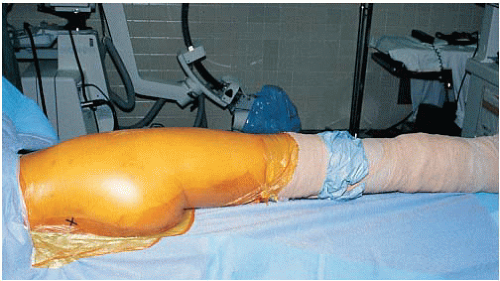 FIGURE 41.14 Patient from Figure 41.10 after sterile preparation and draping. The posteriorsuperior iliac spine is marked with an “X.” The right leg is draped free.
Related posts: Intra-Articular Fractures of the Distal Humerus: Total Elbow Arthroplasty
Humeral Shaft Fractures: Open Reduction Internal Fixation
Distal Humerus Fractures: Open Reduction Internal Fixation
Tarsometatarsal Lisfranc Injuries: Evaluation and Management
Ankle Fractures
Patella Fractures: Open Reduction Internal Fixation Intra-Articular Fractures of the Distal Humerus: Total Elbow Arthroplasty
Humeral Shaft Fractures: Open Reduction Internal Fixation
Distal Humerus Fractures: Open Reduction Internal Fixation
Tarsometatarsal Lisfranc Injuries: Evaluation and Management
Ankle Fractures
Patella Fractures: Open Reduction Internal Fixation
Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

|