Harrison Model
Lantz Model
Vertebral subluxation is at the core of chiropractic theory, and its detection, management, and correction is at the heart of chiropractic practice. This central defining principle is simultaneously a source of debate within the profession. 1 In chiropractic’s first century, subluxation was defined predominately in structural terms23456 and 7 and has evolved from a simplistic static concept, interpreted as a malpositioned spinal segment (bone out of place), to a contemporary model presented as a dynamic and complex biomechanical entity of multiple components. The components of the dynamic model include abnormal joint motion, muscular and connective tissue changes, and vascular, inflammatory, and biochemical changes. In addition, a most significant component of this entity, the associated neurologic manifestations, may result in symptoms either locally or at segmentally innervated anatomic levels (i.e., dermatomes, myotomes) far distant from the point of vertebral dysfunction. The orthopedist Jackson states that mechanical derangement or inflammation of these spinal joints may cause pain, sensory and motor disturbances, or both anywhere along the segmental distribution of the nerves. 8 The neurologic component of the vertebral subluxation complex (VSC) provides chiropractors the potential to move beyond symptomatic treatment of low back pain and other musculoskeletal ailments and to contribute to patient health, wellness, and enhanced function and quality of life.
The term subluxation comes from the Latin sub, meaning under or less than, and luxation, which means dislocation. Stedman’s Medical Dictionary defines the term as “an incomplete luxation or dislocation; though a relationship is altered, contact between joint surfaces remains.”9 Contemporary interpretation embraces the concept of subluxation as a motion segment in which alignment, movement integrity, physiologic function, or any combination is altered, although contact between joint surfaces remains intact. 10
Application of this term is fundamental to communication between chiropractors and their patients. For explaining the subluxation to laypeople, a good working definition is loss of proper motion or position of a vertebral joint that may affect proper nerve function11. In contrast, the term may be described technically as the vertebral subluxation complex and presented as a theoretical model of vertebral motion segment dysfunction that incorporates the complex interactions of pathologic changes in nerve, muscle, ligamentous, vascular, and connective tissue. 12 This latter model serves as a basis for communicating chiropractic concepts to the scientific community.
Classical and contemporary medical practitioners, osteopaths, and chiropractors have referred to the concept of subluxation extensively. 13 However, these professions differ on defining the term and interpreting its clinical significance. In the scientific literature, the terminology describing the functional or structural disorders of synovial joint structures has varied in name and description, ranging from the orthopedic context as a partial or incomplete dislocation to the chiropractic perspective that includes minor misalignment of articulations, hypomobile spinal segments, or both. 13Box 7-1, from Peterson and Bergman, 14 provides an overview of contemporary terminology describing synovial joint dysfunction.
Box 7-1
TERMS DESCRIBING FUNCTIONAL OR STRUCTURAL DISOMRDERS OF THE SYNOVIAL JOINTS
ORTHOPEDIC SUBLUXATION
This term is used to describe a partial or incomplete dislocation.
CHIROPRACTIC SUBLUXATION
This term is used to describe the alteration of the normal dynamic, anatomic, or physiologic relationships of contiguous articular structures; a motion segment in which alignment, movement integrity, or physiologic function is altered, although the contact between the joint surfaces remains intact; an aberrant relationship between two adjacent articular structures that may have functional or pathologic sequelae, causing an alteration in the biomechanical or neurophysiologic reflections of these articular structures or body systems that may be directly or indirectly affected by them.
SUBLUXATION SYNDROME
This term is used to describe an aggregate of signs and symptoms that relates to the pathophysiology or dysfunction of spinal and pelvic motion segments or to the peripheral joints.
SUBLUXATION COMPLEX
This term is used to describe a theoretic model of motion segment dysfunction (subluxation) that incorporates the complex interaction of pathologic changes in nerve, muscle, ligamentous, vascular, and connective tissues.
JOINT DYSFUNCTION
This term is used to describe joint mechanics that show area disturbances of function without structural change—subtle joint dysfunctions that affect quality and range-of-joint motion. Definition embodies disturbances in function that can be represented by decreased motion, increased motion, or aberrant motion.
Joint hypomobility: Decreased angular or linear joint movement
Joint hypermobility: Increased angular or linear joint movement; aberrant joint movements are typically not present
Clinical joint instability: Increased linear and aberrant joint movement; the instantaneous axes of rotation (centroids) and patterns of movement that are disturbed
SOMATIC DYSFUNCTION
This term is used to describe impaired or altered function of related components of the somatic (body framework) system; skeletal, arthrodial, and myofascial structures; and related vascular, lymphatic, and neural elements.
OSTEOPATHIC LESION
This term is used to describe a disturbance in musculoskeletal structure or function, as well as accompanying disturbances of other biologic mechanisms. This term is also used to describe local stress or trauma and subsequent effects on other biologic systems (e.g., effects mediated through reflex nerve pathways, including autonomic supply of segmentally related organs).
JOINT FIXATION
This term is used to describe the state whereby an articulation has become temporarily immobilized in a position that it may normally occupy during any phase of physiologic movement; the immobilization of an articulation in a position of movement when the joint is at rest or in a position of rest when the joint is in movement.
From Peterson D, Bergman T: Chiropractic technique: principles and procedures, ed 2, St Louis, 2002, Mosby.
Rome, 15 in an extensive literature review, has identified over 296 synonyms (41 used to describe sacroiliac subluxation) and terms for the biomechanical condition known to chiropractors as subluxation. Such synonyms include manipulable spinal lesion, functional spinal lesion, dysfunctional segmental unit, somatic joint dysfunction, articular dyskinesia, joint blockage, hypomobile vertebral segment, and vertebral fixation. As an example, Seaman16,17 proposes the term joint complex dysfunction to embrace pathologic and functional changes in a joint, including negative effects of hypomobility-immobility, functional imbalances of muscle tightening or shortening, and myofascial trigger points. Lack of uniform terminology, however, has created confusion and impeded interprofessional discussion.
One way to review the basic principles of spinal adjustment-manipulation is to look at the clinical characteristics of the entity to which the adjustment or manipulation is applied. Despite the various theoretical explanations for the mechanism of action of spinal adjustment/manipulation (see Chapter 8 for greater detail), substantial agreement exists on certain fundamental clinical characteristics of the manipulable lesion or joint subluxation. 18 This chapter explores various aspects of the theoretical models of vertebral subluxation.
SUBLUXATION: EARLY HISTORY
The earliest concepts of subluxation predate chiropractic by more than 200 years. Haldeman cites the earliest English definition of subluxation from Randle Holme in 1688, 19 who described it as, “dislocation or putting out of joynt.”
Haldeman13 and others2021 and 22 cite the following 1746 description from Joannes Herricus Hieronymus, 23 who wrote, “subluxation of joints is recognized by lessened motion of the joints, by slight change in position of the articulating bones and pain.”
Terrett24 cites an 1821 description by Edward Harrison:
When any of the vertebrae become displaced or too prominent, the patient experiences inconvenience from a local derangement in the nerves or the part. He, in consequence is tormented with a train of nervous symptoms, which are obscure in their origin as they are stubborn in their nature.
Harrison pursued the subject further, writing in 1824 that motion, as well as alignment, played a defining role in subluxation:
The articulating extremeties are only partially separated, not imperfectly disjoined … and … the articular motions are imperfectly performed, because the surfaces of the bones do not fully correspond.
Thomas Brown, writing in the Glasgow Medical Journal in 1828, coined the term spinal irritation. 25 Four years later, The American Journal of Medical Sciences began citing reports from European physicians about tenderness of vertebrae corresponding to diseased organs, with such observations taken as confirming a diagnosis of spinal irritation. 25
Donald Tower26 quotes physician J.E. Riadore’s 1843 Irritation of the Spinal Nerves as follows: “[If] any organ is deficiently supplied with nervous energy or of blood, its functions immediately, and sooner or later its structure, becomes deranged.” Riadore concluded that irritation of nerve roots resulted in disease and advocated treatment by manipulation. These conclusions regarding nerve irritation were published 2 years before the birth of D.D. Palmer. 21
By 1874, Andrew Taylor Still, a medical physician who founded osteopathy 21 years before Palmer’s discovery of chiropractic, developed his own concept and terminology. Still described the osteopathic lesion in terms of pressure applied by muscles to blood vessels coursing through and around these muscles, thereby shutting off the life force of the involved tissue. 27
CHIROPRACTIC SUBLUXATION—EARLY CONCEPTS
Although the founder of chiropractic, D.D. Palmer, continued to modify his early concepts and explanations of chiropractic even until his death in 1913, 28 the sustaining, central Palmer hypothesis described subluxation as a “partial or incomplete separation, one in which the articulating surfaces remain in partial contact.”29 His hypothesis further proposed that such subluxations might impinge on spinal nerve roots as they exit through the intervertebral foramina. This action was postulated to obstruct flow of vital nerve impulses between the central nervous system and the periphery and to induce lowered tissue resistance and disease in the segmentally innervated tissues. 2,3,30 The founder later postulated that the primary cause of disease was interruption of normal tone resulting from subluxation, in which nerves became too taut (resulting in excess nerve energy) or too slack (producing too little nerve energy).2829 and 30
In the December 1904 Palmer School of Chiropractic periodical, The Chiropractor, presented as “A monthly journal devoted to the interests of chiropractic—’KI-RO-PRAK-TIK,”31 D.D. Palmer states:
Ninety-five percent of all deranged nerves are made by sub-luxations of vertebrae which pinch nerves to some one of the 51 joint articulations of the spinal column. Therefore to relieve the pressure upon these nerves means to restore normal action—hence, normal functions, perfect health.
This statement likely represents the earliest published mention of subluxation in the chiropractic literature. Significantly, the senior Palmer saw at least limited value (5%) in the adjustment of nonspinal articulations, stating that nerves related to nonvertebral joints may be impinged rather than pinched.
According to Gibbons, 32Modernized Chiropractic, 33 by Smith, Langworthy, and Paxson, published in 1906, was the first chiropractic textbook to use the term subluxation and to relate it to the intervertebral foramen. This work was also the first to assert the supremacy of the nerves in relation to health and disease, in contrast to the osteopathic concept of supremacy of the blood. In chiropractic’s early years, this citation often served as legal defense in arguing the distinction between the practice of chiropractic and that of osteopathy and medicine. In addition, chiropractic’s focus on the importance of the nervous system and its emphasis on the correction of vertebral subluxation became key factors in defending chiropractors and in early attempts by the profession to gain separate licensure.
Langworthy and colleagues also were the first to characterize subluxation as a fixation and to describe the field of motion of a vertebra. This view of subluxation as a dysfunctional state of vertebral motion gradually fell into disuse until 1938, when the dynamic concept of subluxation was reintroduced with the motion palpation research of the Belgian chiropractors Gillet and Lichens. 34
FOUNDER’S DEFINITION
In 1910, D.D. Palmer discussed subluxation in his text, Science, Art and Philosophy of Chiropractic, 2 as follows:
A vertebra is said to be displaced or a luxation when the joint surfaces are entirely separated. Sub-luxation is a partial or incomplete separation; one in which the articulation surfaces remain in partial contact. This later condition is so often referred to and known by chiropractors as sub-luxation. The relationship existing between bones and nerves are so nicely adjusted that any one of the 200 bones, more especially those of the vertebral column, cannot be displaced ever so little without impinging upon adjacent nerves. Pressure on nerves excites, agitates, creates an excess of molecular vibration, whose effects, when local are known as inflammation, when general, as fever. A subluxation does not restrain or liberate vital energy. Vital energy is expressed in functional activity. A subluxation may impinge against nerves, the transmitting channel may increase or decrease the momentum of impulses, not energy.
THE YOUNGER PALMER’S DEFINITION
By the early 1930s, B.J. Palmer had developed a concept of subluxation distinct from that of his father. The younger Palmer represented subluxation as restricted to a displaced upper cervical vertebra that created nerve impingement, resulting in interference with the transmission of vital nerve energy. 3 In his 1934 textbook, The Subluxation Specific—The Adjustment Specific, B.J. maintained that the only subluxation of significance was that of the atlas vertebra in relation to occiput or axis:
I reaffirm that no amount of “adjusting” upon any, many or all vertebrae below occiput, atlas, or axis, could or would directly ADJUST THE SPECIFIC three-direction torqued subluxation causing any, many or all sickness in a body. Any vertebra below atlas or axis MAY BE misaligned but CANNOT BE SUBLUXATED. 3 [Emphasis in original text.]
B.J. Palmer’s delineation between simple misalignment and true subluxation is significant. Misalignment of a vertebra was described as no more than compensation to the major subluxation.
Thus in a span of 30 years, the Palmer School concept of subluxation and adjustment evolved from the founder’s 1904 description of an entity affecting any of the 200 joints of the body, but primarily the joints of the spinal column, to the younger Palmer’s insistence on exclusive adjustment of the full spinal column only and then later to his idea that subluxation was an entity limited only to the atlas vertebra in relation to the occiput and axis. This later concept, known as the Hole in One Technique (HIO), was developed in the early 1930s. For two decades, Palmer College taught no adjusting methods except upper cervical specific technique. Not until 1956 did the school reintroduce instruction in adjusting techniques for the full spine (Himes HM, Policy Talk, unpublished letter, January 4, 1956).
STEPHENSON’S DEFINITION
According to Lantz, 35 the definition of subluxation most widely quoted by early chiropractors was from R.W. Stephenson’s 1927 Chiropractic Text Book, 4 which states:
A subluxation is a condition of a vertebra that has lost its proper juxtaposition with the one above or the one below, or both; to an extent less that a luxation; which impinges nerves and interferes with the transmission of mental impulses.
Stephenson, a 1921 Palmer School graduate, insisted that nerve interference must exist to qualify the condition as a subluxation. Stephenson’s definition served for decades as the preeminent expression of the static model (bone out of proper position or alignment) of vertebral subluxation.
DYNAMIC MODEL
Beginning with the writings of Gillet, 34 Illi, 36 and Mennell, 37 and continuing through the works of Sandoz, 38 Dishman, 39 and Faye, 40 the dynamic characteristics of joint subluxation moved to the forefront, with subluxation and joint integrity now described not solely in structural terms, but in functional terms as well with emphasis on altered joint motion. In this context, joint malposition became a potential sign of altered joint function, but not absolute confirmation. 14
CONTEMPORARY DEFINITIONS
Contemporary definitions describe the subluxation as central to the principles of chiropractic science. Examples of policy statements regarding subluxation are the following:
State Statutes
The concept of subluxation is specifically identified in many U.S. state statutes defining the practice of chiropractic. After extensive review, Hendrickson41 concluded that many state chiropractic statutes either directly or implicitly identify chiropractic with subluxation or the elements of subluxation complex and specify the doctor of chiropractic’s responsibility for adjusting the spine and adjacent tissues for the purpose of eliminating nerve interference. An analysis by Hendrickson follows.
Examples of state statutes that expressly identify the detection of and caring for subluxations as the core of chiropractic practice include:
Arizona: A doctor of chiropractic is a portal of entry health care provider who engages in the practice of health care that includes: the diagnosis and correction of subluxations, functional vertebral or articular dysarthrosis or neuromuscular skeletal disorders for the restoration and maintenance of health.
Treatment by adjustment of the spine or bodily articulations and those procedures preparatory and complementary to the adjustment including physiotherapy related to the correction of subluxations. (Arizona Revised Statutes Annotated, Title 32, Chapter 8, Article 2 32-925(a), No. 1, 3)
Connecticut: The practice of chiropractic means the practice of that branch of the healing arts consisting of the science of adjustment, manipulation and treatment of the human body in which vertebral subluxations and other malpositioned articulations and structures that may interfere with the normal generation, transmission and expression of nerve impulse between the brain, organs and tissue cells of the body, which may be a cause of disease, are adjusted, manipulated or treated. (Connecticut General Statutes Annotated, Title 20, Chapter 372, Section 20-24, (1))
District of Columbia: “Practice of Chiropractic” means the detecting and correcting of subluxations that cause vertebral, neuromuscular, or skeletal disorder, by adjustment of the spine or manipulation of bodily articulations for the restoration and maintenance of health. (District of Columbia Code 1981, Part 1, Title 2, Chapter 33, Subchapter I -2-3301.2(3)(A))
Delaware: The practice of chiropractic includes, but is not limited to, the diagnosing and locating of misaligned or displaced vertebral subluxation complex. (Delaware Code Annotated, Title 24, Chapter 7, 701 b.)
Florida: “Practice of chiropractic” means a noncombative principle and practice consisting of the science, philosophy, and art of the adjustment, manipulation, and treatment of the human body in which vertebral subluxations and other malpositioned articulations and structures that are interfering with the normal generation, transmission, and expression of nerve impulse between the brain, organs, and tissue cells of the body, thereby causing disease, are adjusted, manipulated, or treated, thus restoring the normal flow of nerve impulse which produces normal function and consequent health by chiropractic physicians using specific chiropractic adjustment or manipulation techniques…. (Florida Statutes Annotated, Title XXXII, Chapter 460, Section 460.403 (8) (a))
Idaho: “Adjustment” means the application of a precisely controlled force applied by hand or by mechanical device to a specific focal point on the anatomy for the express purpose of creating a desired angular movement in skeletal joint structures in order to eliminate or decrease interference with neural transmission and correct or attempt to correct subluxation complex. (Idaho Code, Title 54 Chapter 7, 54-704 (1) (a))
Maine: Chiropractic. “Chiropractic” means the art and science of identification and correction of subluxation and the accompanying physiological or mechanical abnormalities. The term subluxation, as utilized within the chiropractic health care system, means a structural or functional impairment of an intact articular unit. Chiropractic recognizes the inherent recuperative capability of the human body as it relates to the spinal column, musculo-skeletal and nervous system. (Maine Revised Statutes Annotated, Title 32, Chapter 9, Subchapter 1, Section 451 (1))
New York: The practice of the profession of chiropractic is defined as detecting and correcting by manual or mechanical means structural imbalance, distortion, or subluxations in the human body for the purpose of removing nerve interference and the effects thereof, where such interference is the result of or related to distortion, misalignment or subluxation of or in the vertebral column. (Consolidated Laws of New York, Chapter 16, Title VIII, Article 132, Section 6551 (1))
Other state statutes that define and identify the subluxation specifically include Kentucky, Nevada, New Jersey, Texas, Utah, Vermont, and Washington.
Medicare and Medicaid Definition
The U.S. government recognizes the detection and correction of subluxation as the primary function of the doctor of chiropractic. 41,42 The federal statutes governing the Medicare program, in which chiropractic services have been included since the early 1970s, defines chiropractic and reimbursable chiropractic services as:
A chiropractor who is licensed as such by the State (or in a State which does not license chiropractors as such, is legally authorized to perform the services of a chiropractor in the jurisdiction in which he performs such services), and who meets uniform minimum standards promulgated by the Secretary, but only for the purpose of subsections (s)(1) and (s)(2)(A) of this section and only with respect to treatment by means of manual manipulation of the spine (to correct a subluxation) which he is legally authorized to perform by the State or jurisdiction in which such treatment is provided. (42 USC Sec. 1395× (r) (5))
Medicare extends these concepts in the statute into the regulations governing the program with an express definition:
A chiropractor who is licensed by the State or legally authorized to perform the services of a chiropractor, but only with respect to treatment by means of manual manipulation of the spine to correct a subluxation. (42 CFR 482 Subpart B Section 482.12 (7) (c) (1) (v))
Federal statutes establishing chiropractic participation in the Medicaid program employ the same terminology as that in the general Medicare program. Federal employee health benefit programs recognize chiropractic on terms negotiated between representative committees of public employees and various insurance carriers, but the federal workers compensation program identifies and defines chiropractic, once again, very specifically to include chiropractors and chiropractic services as follows:
The term “physician” includes chiropractors only to the extent that their reimbursable services are limited to treatment consisting of manual manipulation of the spine to correct a subluxation.
Department of Veterans Affairs
In January 2002, President George W. Bush signed into law new provisions that established chiropractic services as a health care benefit for eligible military veterans in the United States. This law contains a specific passage referencing subluxation, which reads as follows41:
Program For The Provision of Chiropractic Care and Services to Veterans. (d) CARE AND SERVICES AVAILABLE. The chiropractic care and services available under the program shall include a variety of chiropractic care and services for neuro-musculoskeletal conditions, including subluxation complex. (United States Code, Title 38, 204 (d))
World Health Organization Classification
The World Health Organization (WHO), a multilateral health care agency of the United Nations, has accepted subluxation as a listing in the International Classification of Diseases, 43referring to it as “M99.1 Subluxation complex (vertebral).” WHO also recognizes the classification “M99.0 Segmental and somatic dysfunction,” a subtle variation.
Consortium for Chiropractic Research
The 1993 consensus definition of the nominal and Delphi panels of the Consortium for Chiropractic Research (CCR) 10 refers to subluxation as “…a motion segment in which alignment, movement integrity, and/or physiologic function are altered although contact between the joint surfaces remains intact.”
American Chiropractic Association
The Indexed Synopsis of ACA Policies44 describes subluxation as, “…[a] motion segment, in which alignment, movement integrity, and/or physiological function are altered although contact between joint surfaces remain intact.”
ACA has also adopted the consensus definitions agreed on by the nominal and Delphi panels of the CCR10,44:
Subluxation is an aberrant relationship between two adjacent articular structures that may have functional or pathological sequelae, causing an alteration in the biomechanical and/or neurophysiological reflections of these articular structures, the proximal structures, and/or body systems that may be directly or indirectly affected by them.
The ACA-endorsed CCR definition44 for subluxation complex is:
…[a] theoretical model of motion segment dysfunction (subluxation) which incorporates the complex interaction of pathological changes in nerve, muscle, ligamentous, vascular and connective tissues.
International Chiropractors Association
ICA Policy Statements45 related to subluxation include the following:
Of primary concern to chiropractic are abnormalities of structure or function of the vertebral column known clinically as the vertebral subluxation complex. The subluxation complex includes any alteration of the biomechanical and physiological dynamics of contiguous spinal structures which can cause neuronal disturbances…. Directly or indirectly, all bodily function is controlled by the nervous system, consequently a central theme of chiropractic theories on health is the premise that abnormal bodily function may be caused by interference with nerve transmission and expression due to pressure, strain or tension upon the spinal cord, spinal nerves, or peripheral nerves as a result of displacement of spinal segments or other skeletal structures (subluxation).
The vertebral subluxation syndrome and/or complex and its component parts is any alteration of the biomechanical and physiological dynamics of the contiguous structures which can cause neuronal disturbances. 46
The science of chiropractic deals with the relationship between the articulations of the skeleton and the nervous system and the role of this relationship in the restoration and maintenance of health. Of primary concern to chiropractic are abnormalities of structure or function of the vertebral column known clinically as the vertebral subluxation complex. The subluxation complex includes any alteration of the biomechanical and physiological dynamics of contiguous spinal structures which can cause neuronal disturbances.
According to the ICA Official Policy Handbook45:
Chiropractic is based on the premises that the relationship between structure and function in the human body is a significant health factor and that such relationships between the spinal column and nervous system are the most significant, since the normal transmission and expression of nerve energy is essential to the restoration and maintenance of health.
Association of Chiropractic Colleges
On July 1, 1996, presidents of all North American chiropractic colleges, as members of the Association of Chiropractic Colleges (ACC), seeking to clarify professional common ground and define chiropractic’s role within the health care delivery system, generated a series of consensus position statements. 47 This effort represented the first time in the 100-year history of chiropractic education that all college presidents, representing schools with diverse institutional missions, have reached unanimous consensus on common core definitions fundamental to the principles of chiropractic. This paradigm is endorsed by the ACA, ICA, World Chiropractic Alliance, World Federation of Chiropractic, the Congress of Chiropractic State Associations, and most state chiropractic associations. This consensus therefore represents a common platform from which to communicate the unifying principles of this profession. Chapter 2, “The Chiropractic Paradigm,” provides the ACC paradigm in its entirety.
ACC CONSENSUS DEFINITIONS
On chiropractic:
Chiropractic is a health-care discipline which emphasizes the inherent recuperative powers of the body to heal itself without the use of drugs or surgery.
The practice of chiropractic focuses on the relationship between structure (primarily of the spine) and function (as coordinated by the nervous system) and how that relationship affects the preservation and restoration of health.
Doctors of Chiropractic recognize the value and responsibility of working in cooperation with other health care practitioners when in the best interest of the patient.
The ACC continues to foster a unique, distinct chiropractic profession that serves as a health care discipline for all. The ACC advocates a profession that generates, develops, and utilizes the highest level of evidence possible in the provision of effective, prudent and cost-conscious patient evaluation and care.
On subluxation:
A subluxation is a complex of functional, structural, and/or pathological articular changes that compromise neural integrity and may influence organ system function and general health.
A subluxation is evaluated, diagnosed and managed through the use of chiropractic procedures based on the best available rational and empirical evidence.
The preservation and restoration of health is enhanced through the correction of the subluxation.
CONTEMPORARY MODELS OF VERTEBRAL SUBLUXATION COMPLEX
As noted in the ACA and ICA definitions previously cited, the contemporary concept of subluxation has been expanded beyond a joint phenomenon affecting nerve function to also include the role of muscular, connective, vascular, and biochemical components as part of a complex. This subluxation complex has been defined by Gatterman20 as “a theoretical model of motion segment dysfunction (subluxation) that incorporates the complex interaction of pathologic change in nerve, muscle, ligamentous, vascular and connective tissues.”
Although Janse, 48,49 Illi, 36 Gillet and Lichens, 34 and Homewood50 provided an early foundation, Faye, 40 beginning in 1967, popularized the concept of the subluxation complex and organized a five-component model. Dishman39 characterized the concept as the chiropractic subluxation complex, providing additional rationale for Faye’s model. Lantz22,35 modified the original five components of the VSC model by postulating three more components: connective tissue pathologic finding, vascular abnormalities, and the inflammatory response.
FIVE-COMPONENT MODEL OF VERTEBRAL SUBLUXATION COMPLEX (FAYE MODEL)
Building on the work of Gillet and Liekens, 34 as well as earlier pioneers such as Smith, Langworthy, and Paxson, 33 Faye40 moved beyond the static “bone out of place” or “displaced vertebra” theory of subluxation, placing primary emphasis on dynamic vertebral joint motion. Basic movements of spinal segments include rotation about the longitudinal axis, right or left lateral flexion, anterior flexion, posterior extension, and long-axis distention. Factors inhibiting movement in one or more of these directions may cause abnormal translation and rotation, contributing to biomechanic and subsequent physiologic dysfunction and pathologic expressions.
Schafer and Faye51 defined the term fixation as referring to any physical, functional, or psychologic mechanism that produces a loss of segmental mobility within its normal physiologic range of motion. As an example, ankylosis of a joint would be considered a 100% fixation. These authors state that clinically most fixations are in the 20% to 80% range of normal mobility. According to Schafer and Faye, once the chiropractor has identified the hypomobility, adjustive procedures are used to mobilize the fixation. The therapeutic objective is to deliver a dynamic thrust, employing a specific contact and line of drive with the intention of freeing restricted vertebral joint motion altering specific symptomatology.
The Faye model of the vertebral subluxation complex (Fig. 7-1) presents subluxation as a complex clinical entity comprising one or more of the following components: neuropathophysiology, kinesiopathology, myopathology, histopathology, and a biochemical component. A central element of this concept is that subluxation results in pathophysiologic conditions, which can then lead to frank pathologic changes. Moreover, correction of a subluxation is considered to lead to the restoration of normal physiologic processes, thus allowing the reversal of reversible pathologic changes.
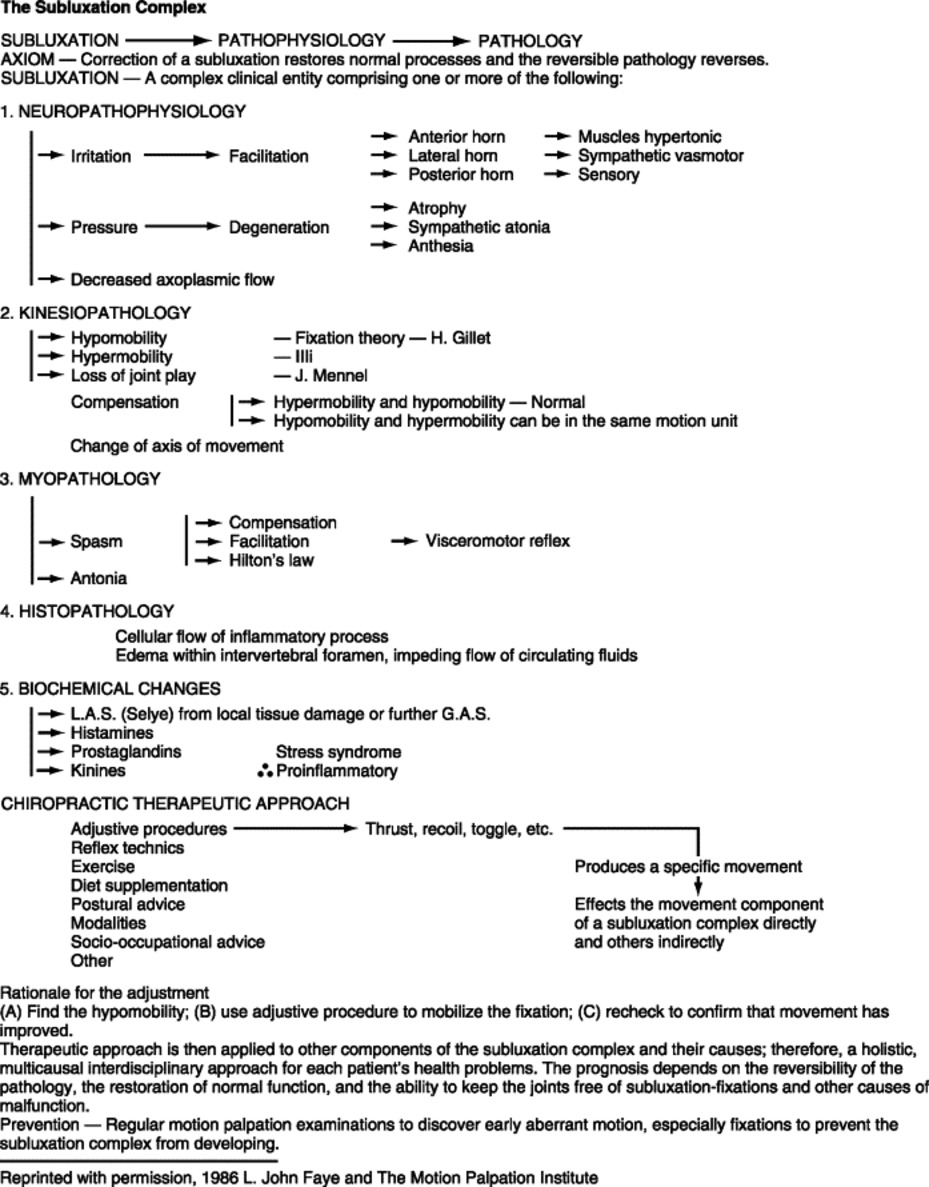 |
| Fig. 7-1 Five-component (Faye) model of subluxation complex. (From Schafer RC, Faye LJ: Motion palpation and chiropractic technic: principles of dynamic chiropractic, Huntington Beach, Calif, 1989, The Motion Palpation Institute, with permission.) |
Specifics of Five-Component Model51
1. Neuropathophysiologic component. Biomechanical insult to nerve tissue is proposed to cause neural dysfunction in three forms, individually or in combination, to include:
a. Irritation (sustained hyperactivity) of nerve receptors or nerve tissue. This irritation results in facilitating (lowering threshold of excitability) of afferent nerve cells (dysafferentation) and evoking activity of efferent neurons with nerve cell bodies located in the anterior horn of the spinal cord, which is exhibited as hypertonicity or spasm of muscles. Lateral horn cell irritation, which is exhibited as vasomotor changes, includes hypersympatheticotonic vasoconstriction. Irritation to the cells of the posterior horn is exhibited as sensory changes.
b. Compression or mechanical insult (pressure, stretching, angulation, or distortion) to neural elements in or about the intervertebral foramina, within fascial layers, or tonically contracted muscles. This compression results in degeneration, which is exhibited as muscular atrophy, anesthesia, and sympathetic atonia, to including hyposympathicotonic vasodilation and vascular stasis.
c. Decreased axoplasmic transport affecting intraaxonal transport mechanisms for delivery of macromolecules (neurotrophic substances). This delivery is via the axon to end organs innervated by the nerve. Impediments to this microcellular transport mechanism may alter the development, growth, and maintenance of cells or structures that are dependent on this trophic (growth) influence expressed via the nerve.
2. Kinesiopathologic component. This component is described as hypomobility, diminished or absent joint play, or compensatory segmental kinematic hypermobility. Lack of appropriate joint motion is proposed to be associated with a variety of nociceptive and mechanoreceptive reflex functions that include proprioception. In addition, an early manifestation of a chronically fixated vertebral articulation is shortening of ligaments as an adaptation to limited range of motion.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


