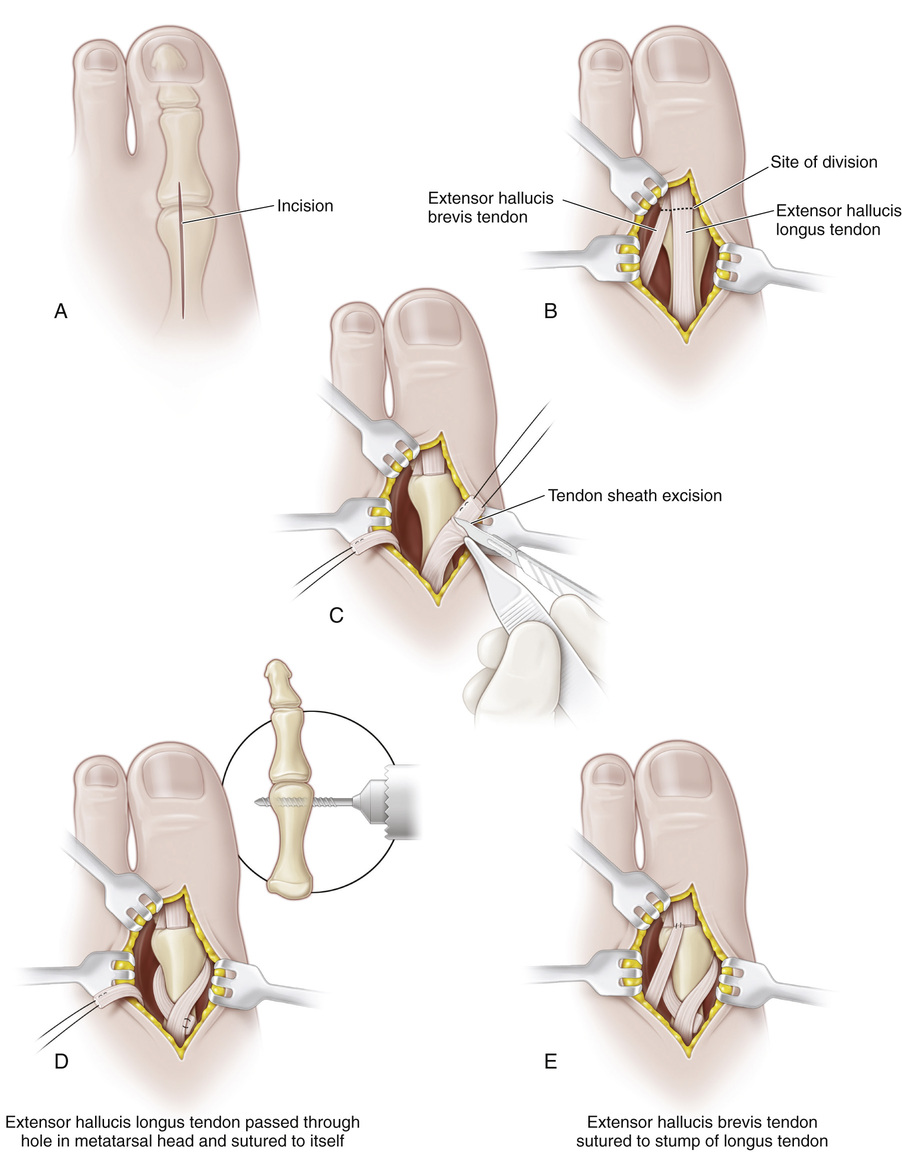
Transfer of the Long Toe Extensors to the Heads of the Metatarsals (Jones Transfer)
A, A longitudinal incision is made on the dorsomedial aspect of the first metatarsal from the base of the proximal phalanx to the proximal fourth of the metatarsal shaft. The incision should be placed medial to the extensor hallucis longus tendon, toward the second metatarsal. The subcutaneous tissue is divided and the wound flaps retracted with 0 silk sutures. The digital nerves and vessels should not be injured.
B, The extensor hallucis longus and brevis tendons are identified and sectioned at the base of the proximal phalanx. An alternative technique is to leave the insertion of the extensor hallucis brevis tendon intact; the stump of the extensor hallucis longus tendon is sutured to the intact brevis tendon.
C, Silk whip sutures (00) are inserted into the ends of the long and short toe extensors. The long toe extensor is dissected free and its sheath is thoroughly excised with a sharp scalpel as far proximally as possible.
D, The epiphyseal plate of the first metatarsal is proximal, whereas that of the lateral four metatarsals is distal in location. The extensor hallucis longus tendon is transferred to the head of the first metatarsal. The long toe extensors of the lesser toes are transferred to the distal third of the metatarsal shafts, with care taken to not disturb the growth plate. When the patient is older than 10 to 12 years, the tendons are transferred to the heads of the metatarsals because by then growth of the foot is almost complete.
With small Chandler elevator retractors, the soft tissues are retracted. The periosteum is not stripped. Through a stab wound in the periosteum, a hole is drilled in the center of the first metatarsal head and enlarged to receive the tendon. The extensor hallucis longus tendon is passed through the hole in the first metatarsal in a medial-to-lateral direction and sutured to itself with the forefoot in maximal dorsiflexion.
E, The extensor hallucis brevis tendon is then sutured to the stump of the long toe extensor while holding the toe in neutral extension or in 10 degrees of dorsiflexion.
A similar technique is used to transfer the long extensor tendons of the lesser toes. Longitudinal incisions are made between the second and third metatarsals and between the fourth and fifth metatarsals. The extensor brevis tendon of the little toe is either absent or not of adequate size to transfer to the stump of the longus.
The tourniquet is released, and complete hemostasis is obtained. The wounds are closed with interrupted sutures.
Postoperative Care
A cast with a sturdy, well-padded toe plate is applied and worn for 4 to 6 weeks. The plantar aspect of the metatarsals should be well padded to prevent ulceration. Special muscle training for the transferred tendons is not required because this is an in-phase transfer.
Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 44 Knee Fusion for Prosthetic Conversion in Proximal Focal Femoral Deficiency
44 Knee Fusion for Prosthetic Conversion in Proximal Focal Femoral Deficiency
 64 Amputation Through the Arm
64 Amputation Through the Arm
 38 Exposure of the Spine for Posterior Instrumentation and Fusion
38 Exposure of the Spine for Posterior Instrumentation and Fusion
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


