Fractional Lengthening of the Finger and Wrist Flexors in the Forearm Operative Technique
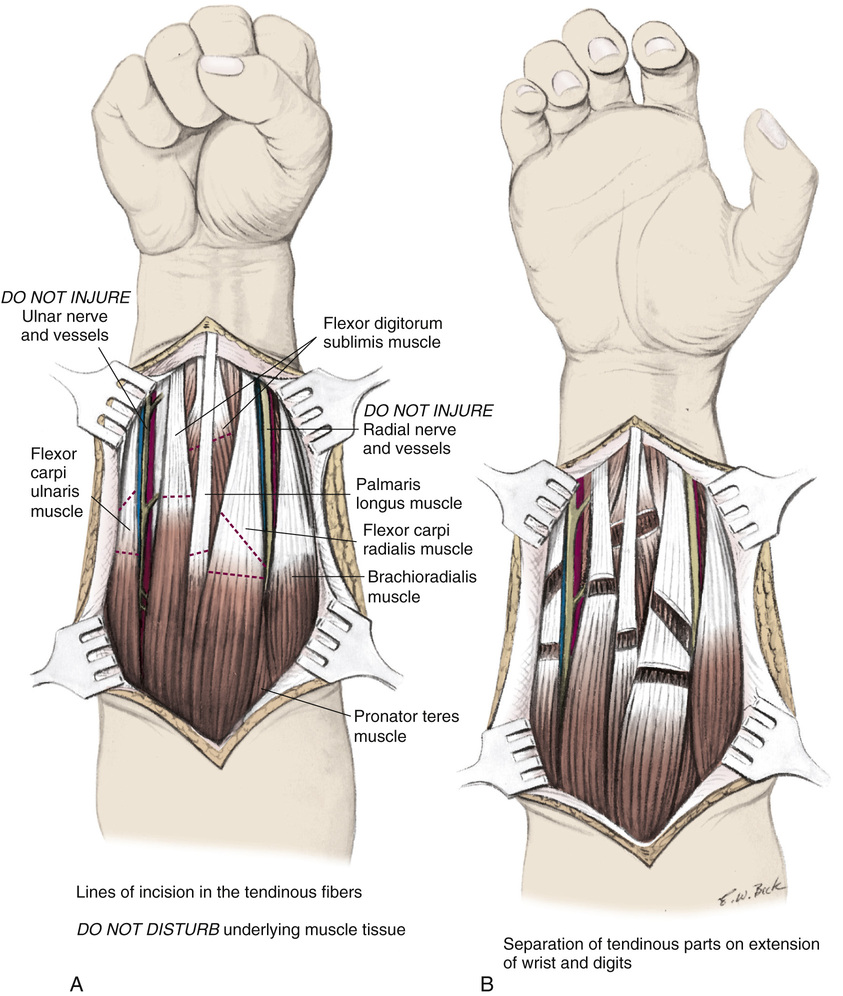
A, A midline longitudinal incision is made in the middle three fourths of the volar surface of the forearm. The subcutaneous tissue and deep fascia are divided in line with the skin incision. The wound flaps are undermined, elevated, and retracted with four-prong rake retractors to expose the superficial groups of muscles. On the radial side of the flexor carpi ulnaris tendon, the ulnar vessels and nerves are identified and protected from injury; similarly, on the radial side of the flexor carpi radialis tendon, the radial vessels and nerve are isolated to protect them from inadvertent damage. Sliding lengthening of the flexor carpi radialis and flexor carpi ulnaris muscles is performed at the musculotendinous junction by making two incisions in their tendinous fibers, about 1.5 cm apart, without disturbing the underlying muscle tissue. The proximal incision is transverse and the distal one is oblique. The palmaris longus and flexor digitorum muscles are lengthened by only one transverse incision in each.
B, The wrist and the fingers are passively hyperextended. The tendinous parts will separate, whereas the intact underlying muscle fibers will maintain continuity of the muscles.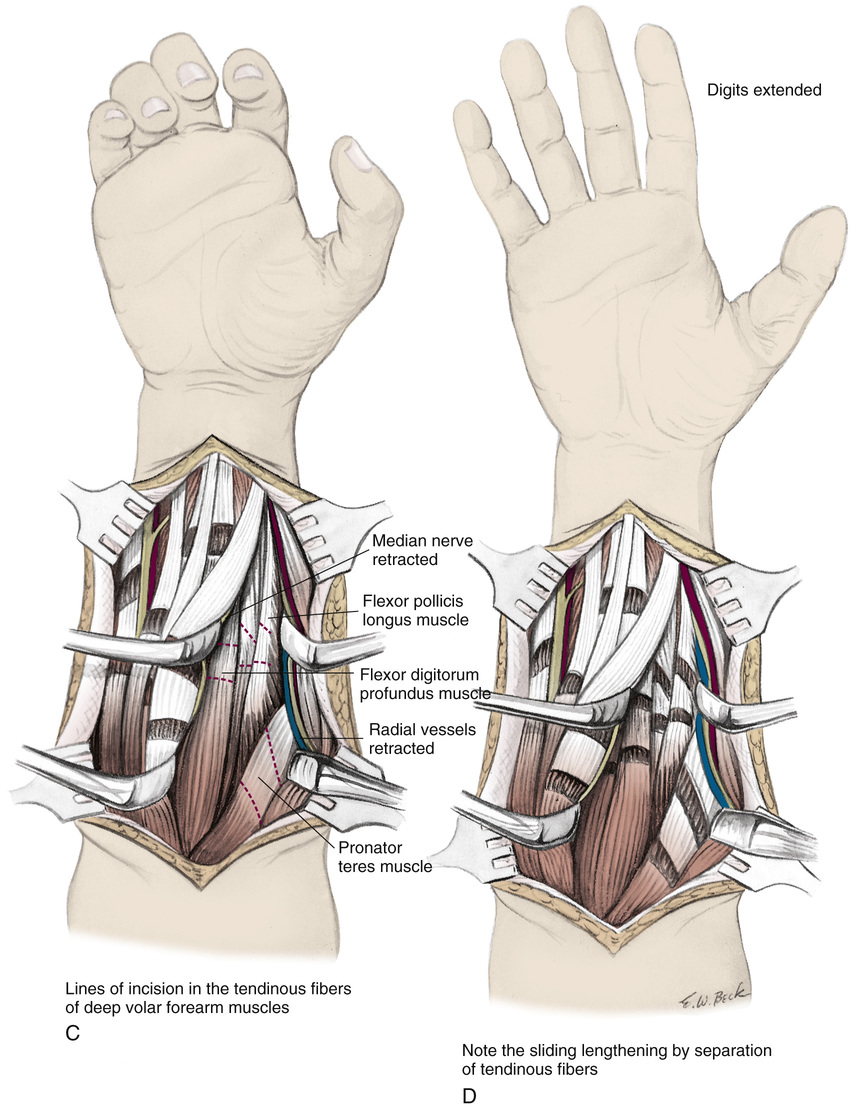
C and D, The deep volar muscles are exposed by retracting the brachioradialis muscle and radial vessels radially and the flexor carpi radialis and flexor digitorum sublimis muscles ulnarward. The median nerve is identified and protected from injury by retracting it medially with the flexor carpi radialis muscle. The flexor pollicis longus and flexor digitorum profundus muscles are lengthened by making two incisions in their tendinous parts and sliding them in the same manner as described for the superficial volar forearm muscles. Continuity of muscles is maintained by gentle handling of tissues and by taking care that adequate muscle substance underlies the divided tendinous parts. Sliding lengthening is achieved by separating the tendinous fibers by slow, but firm extension of the thumb and four ulnar digits.
Next, the range of passive supination of the forearm is tested. If a pronation contracture is present, the pronator teres muscle is lengthened by two oblique incisions, 1.5 cm apart, in its tendinous fibers. Again, the underlying muscle tissue should not be disturbed. The forearm is forcibly supinated; the tendinous segments will slide and separate, thereby elongating the muscle.
The tourniquet is released and complete hemostasis is obtained. The deep fascia is not closed. The subcutaneous tissue and skin are approximated by interrupted sutures. An above-elbow cast that includes all the fingers and the thumb is applied to immobilize the forearm in full supination, the elbow in 90 degrees of flexion, the wrist in 50 degrees of extension, and the fingers and thumb in neutral extension.
Postoperative Care
Four weeks after surgery, the cast is removed and active exercises are started to develop motor power in the elongated muscle. Squeezing soft balls of various size and other functional exercises are carried out several times a day. An aggressive occupational therapy program is essential. The corrected position is maintained in a bivalved cast. As motor function develops in the elongated muscle and its antagonists, periods out of the cast are gradually increased.
Related posts:
 23 Hamstring Lengthening
23 Hamstring Lengthening
 29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
29 Achilles Tendon—Distal Fibular Tenodesis for Mild Ankle Valgus in Skeletally Immature Patients
 44 Knee Fusion for Prosthetic Conversion in Proximal Focal Femoral Deficiency
44 Knee Fusion for Prosthetic Conversion in Proximal Focal Femoral Deficiency
 64 Amputation Through the Arm
64 Amputation Through the Arm
 38 Exposure of the Spine for Posterior Instrumentation and Fusion
38 Exposure of the Spine for Posterior Instrumentation and Fusion
 42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
42 Anterior Instrumentation of the Spine for Thoracolumbar or Lumbar Scoliosis
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


