Chapter 13 Rehabilitation of Primary and Revision Anterior Cruciate Ligament Reconstructions
CLINICAL CONCEPTS
The two anterior cruciate ligament (ACL) postoperative rehabilitation protocols described in this chapter consist of a careful incorporation of exercise concepts supported by the scientific data presented in Chapter 12, Scientific Basis of Rehabilitation after Anterior Cruciate Ligament Autogenous Reconstruction. The protocols are evaluation-based; that is, progression through the program is based on continual evaluation using the principles of anatomy, physiology, biomechanics, and surgery 2–5,7,14–17 and understanding that the overall goals of the reconstruction and rehabilitation are to
 Regain normal knee stability (<3 mm of increased anteroposterior [AP] displacement on knee arthrometer testing, negative or trace pivot shift).
Regain normal knee stability (<3 mm of increased anteroposterior [AP] displacement on knee arthrometer testing, negative or trace pivot shift).









 Concomitant major operative procedures including meniscal repair, ligament reconstruction, patellofemoral realignment, articular cartilage restorative procedure, and osteotomy.
Concomitant major operative procedures including meniscal repair, ligament reconstruction, patellofemoral realignment, articular cartilage restorative procedure, and osteotomy.

 Magnetic resonance imaging (MRI) or arthroscopic evidence of major bone bruising or articular cartilage damage.
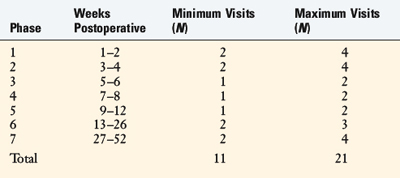
Magnetic resonance imaging (MRI) or arthroscopic evidence of major bone bruising or articular cartilage damage.Specific criteria are evaluated throughout both rehabilitation programs to determine whether the patient is ready to progress from one phase to the next. Both protocols incorporate a home self- management program, along with an estimated number of formal physical therapy visits (Table 13-1). For most patients, 11 to 21 postoperative visits are expected to produce a desirable result. A few more supervised sessions may be required between the 6th and the 12th postoperative month for patients who undergo advanced training to return to strenuous activities. A specific neuromuscular-retraining program (Sportsmetrics) is advocated for all patients returning to high-risk activities, discussed in Chapter 19, Decreasing the Risk of Anterior Cruciate Ligament Injuries in Female Athletes. For all patients, the following signs are continually monitored postoperatively: joint swelling, pain, gait pattern, knee moion, patellar mobility, muscle strength, flexibility, and AP displacement. Any individual who experiences difficulty progressing through the protocol or who develops a complication is expected to require additional supervision in the formal clinic setting.
TABLE 13-1 Estimated Supervised Physical Therapy Visits after Anterior Cruciate Ligament Reconstruction
REHABILITATION PROTOCOL FOR PRIMARY ACL B-PT-B AUTOGENOUS RECONSTRUCTION: EARLY RETURN TO STRENUOUS ACTIVITIES
Modalities
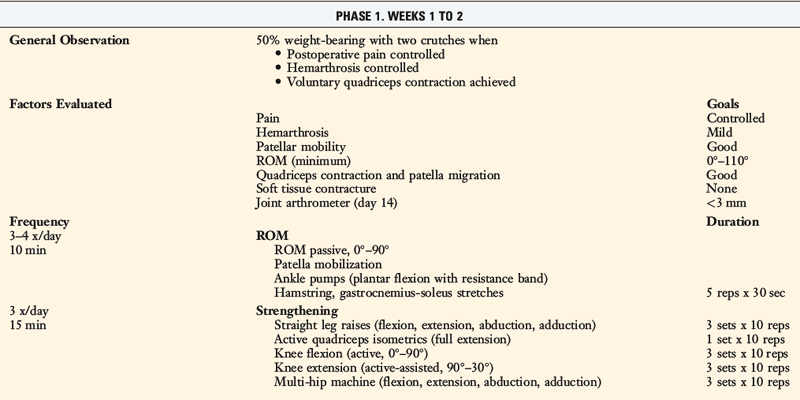
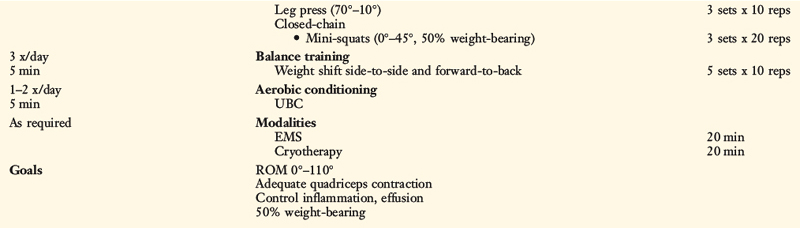
In the immediate postoperative period (1–3 days), knee effusion must be controlled to avoid the quadriceps inhibition phenomenon. Electrogalvanic stimulation or high-voltage electrical muscle stimulation (EMS) may be used to augment the ice, compression, and elevation program to control swelling. This treatment uses the concept of like charges repelling. The effusion or swelling has a negative electrical charge, so using the negative electrodes at the knee and the positive (dispersive) electrode on either the low back or the opposite thigh will assist the body in removing the fluid from the joint to be reabsorbed. The treatment duration is approximately 30 minutes, the intensity is set to patient tolerance, and the treatment frequency is three to six times per day. Once the joint effusion is controlled, functional EMS is begun for muscle reeducation and quadriceps facilitation (Table 13-2).
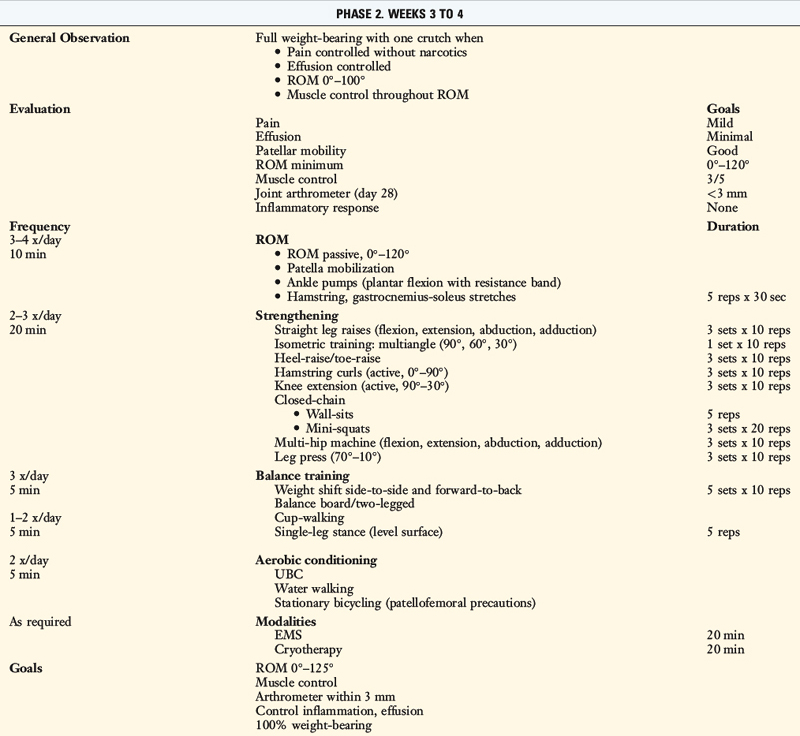
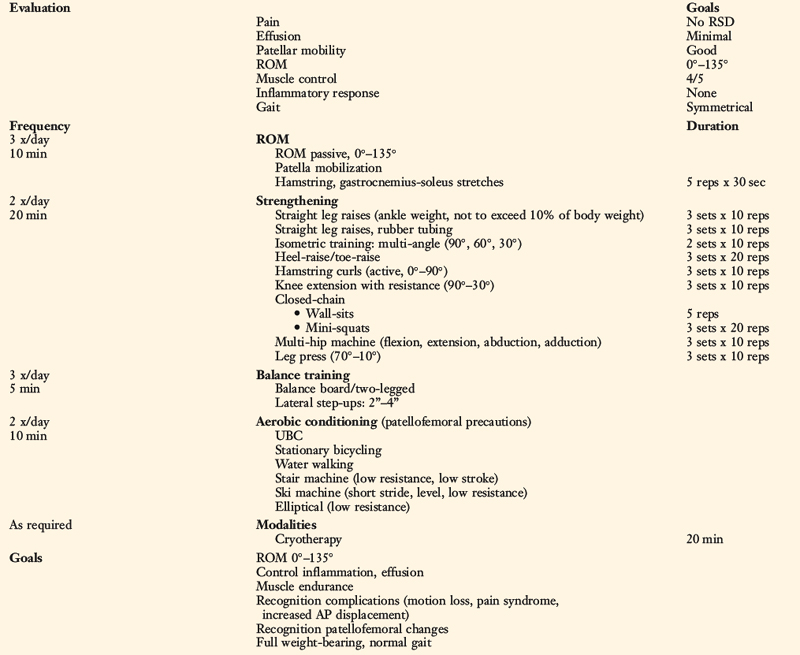
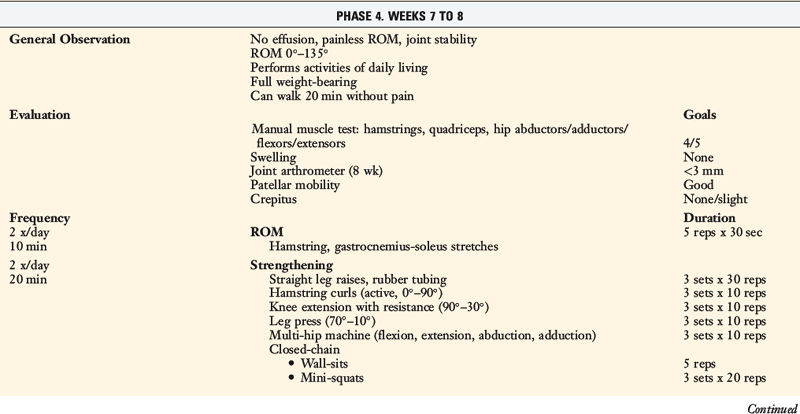
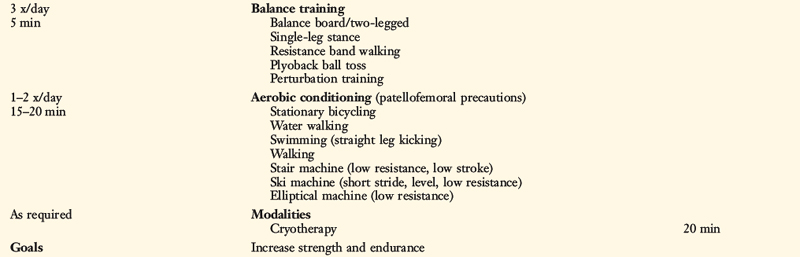
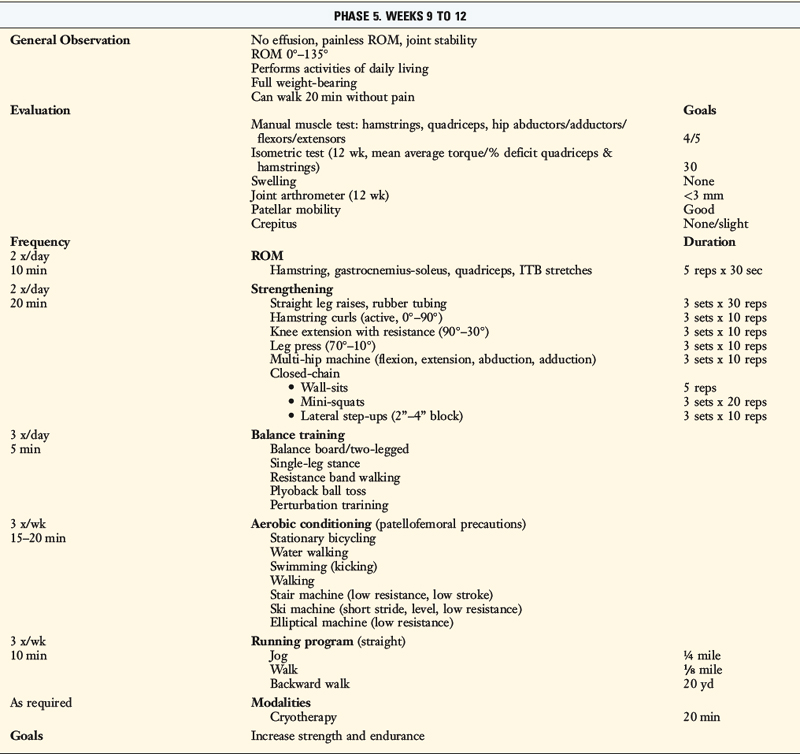
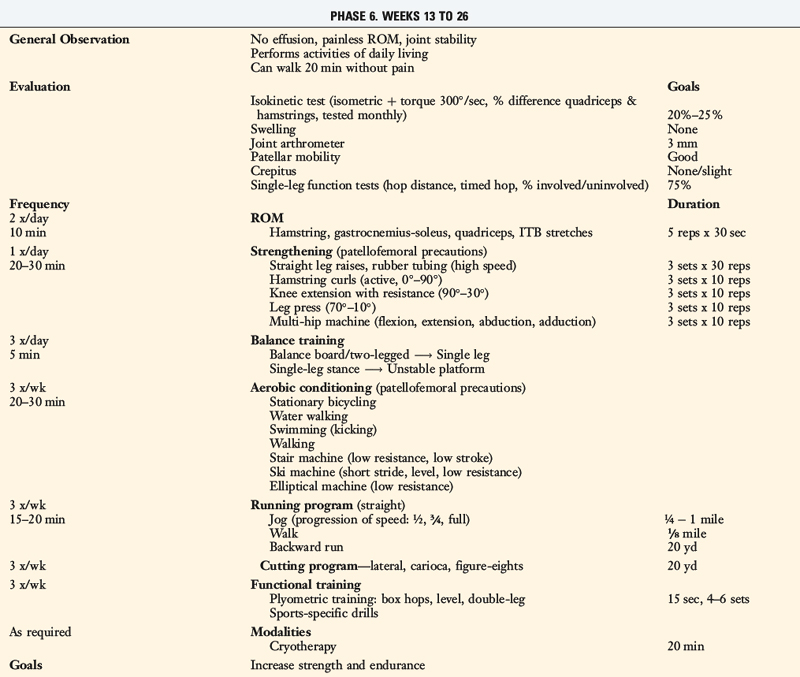
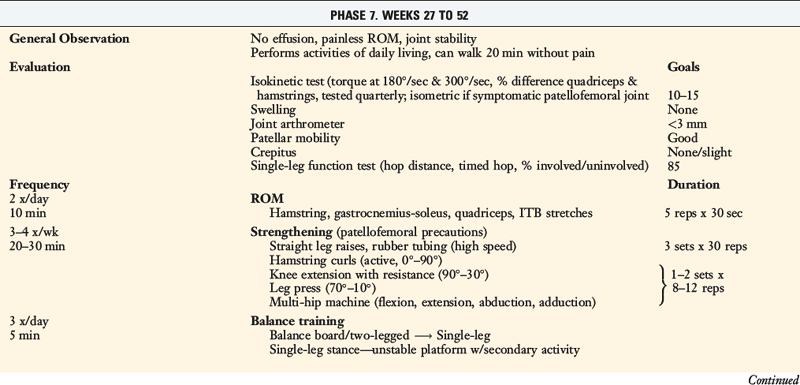
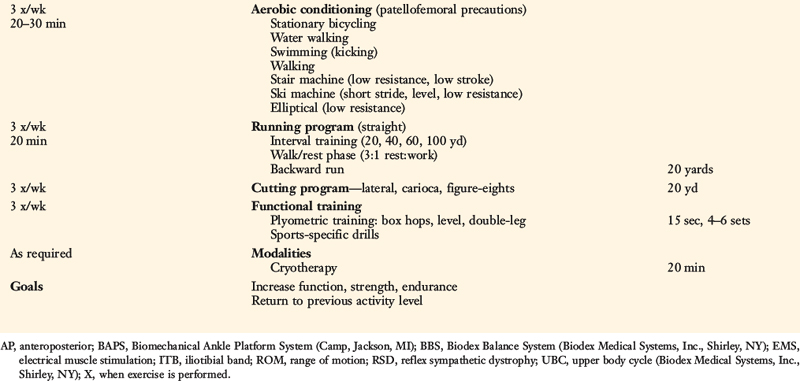
TABLE 13-2 Cincinnati Sportsmedicine and Orthopaedic Center Rehabilitation Protocol for Primary Anterior Cruciate Ligament Reconstruction: Early Return to Strenuous Activities
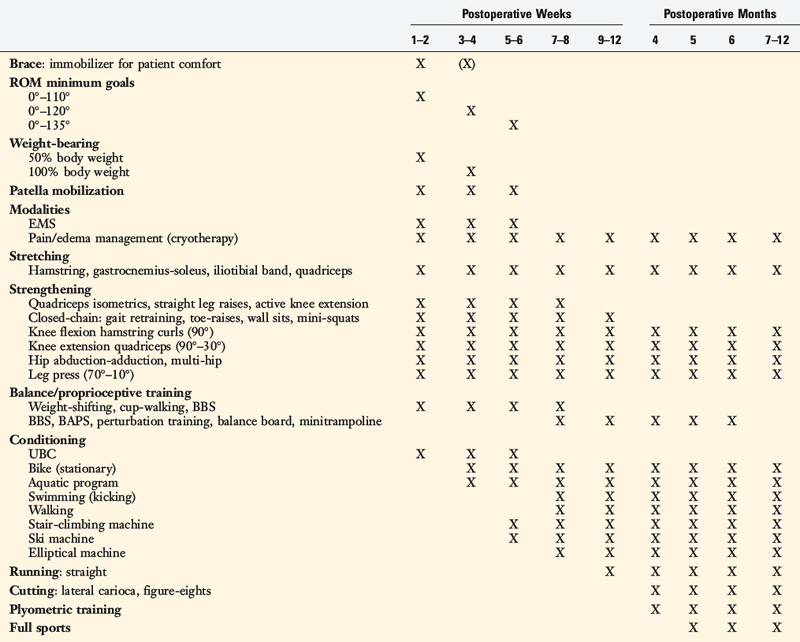

Postoperative Bracing
Range of Knee Motion
Patellar mobilization: all four planes, done with motion exercises.
Partial weight-bearing immediately, full by 3–4 wk.
Flexibility: Hamstring, gastrocnemius-soleus, quadriceps, iliotibial band.
Strengthening
Balance, Proprioception
Running, Agility
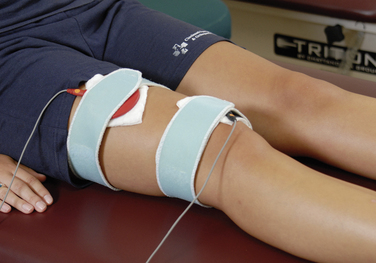
The use of EMS to facilitate and enhance an adequate quadriceps contraction is based on the evaluation of quadriceps and vastus medialis oblique (VMO) muscle tone. One electrode is placed over the VMO and the second electrode is placed on the central to lateral aspect of the upper third of the quadriceps muscle belly (Fig. 13-1). The treatment duration is 20 minutes. The patient actively contracts the quadriceps muscle simultaneously with the machine’s stimulation. A portable EMS machine for home use may be required in individuals whose muscle rating is poor. EMS is continued until the muscle grade is rated as good.
Biofeedback therapy also has an important role in facilitating an adequate quadriceps muscle contraction early postoperatively. The surface electrode is placed over the selected muscle component to provide positive feedback to the patient and clinician regarding the quality of active or voluntary quadriceps contraction (Fig. 13-2). Biofeedback is also useful in enhancing hamstring relaxation if the patient experiences difficulty achieving full knee extension secondary to knee pain or muscle spasm. The electrode is placed over the belly of the hamstring muscle while the patient performs range of motion (ROM) exercises.

The most widely used modality after ACL reconstruction is cryotherapy, which is begun in the recovery room after surgery. Cost of various cryotherapy options and patient compliance are two major factors in the successful control of postoperative pain and swelling. The standard method of cold therapy is an ice bag or commercial cold pack, which is kept in the freezer until required. Empirically, patients prefer motorized cooler units (Fig. 13-3). These units maintain a constant temperature and circulation of ice water through a pad, which provides excellent pain control. Gravity flow units are also effective; however, temperature maintenance is more difficult with these devices than with the motorized cooler units. The temperature can be controlled by using gravity to backflow and drain the water, refilling the cuff with fresh ice water as required. Cryotherapy is used for 20 minutes at a time from three times a day to every waking hour depending upon the extent of pain and swelling. In some cases, the treatment time is extended owing to the thickness of the buffer used between the skin and the device. The motorized units contain a thermostat, which is helpful when cold therapy is used for an extended treatment time. Vasopneumatic devices offer another option for cold therapy. The Game Ready device (Game Ready, Berkeley, CA) allows the clinician to set the temperature and, as well, one of four different compression levels depending on patient tolerance. Although this is primarily a clinical treatment tool, it may be used at home as well. Cryotherapy is typically done after exercise or when required for pain and swelling control and is maintained throughout the entire postoperative rehabilitation protocol.
< div class='tao-gold-member'>

Related posts:
 Human Movement and Anterior Cruciate Ligament Function: Anterior Cruciate Ligament Deficiency and Gait Mechanics
Human Movement and Anterior Cruciate Ligament Function: Anterior Cruciate Ligament Deficiency and Gait Mechanics
 Differences in Neuromuscular Characteristics between Male and Female Athletes
Differences in Neuromuscular Characteristics between Male and Female Athletes
 Rehabilitation after Articular Cartilage Procedures
Rehabilitation after Articular Cartilage Procedures
 Lateral, Posterior, and Cruciate Knee Anatomy
Lateral, Posterior, and Cruciate Knee Anatomy
 Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
Meniscus Transplantation: Diagnosis, Operative Techniques, and Clinical Outcomes
 Primary, Double, and Triple Varus Knee Syndromes: Diagnosis, Osteotomy Techniques, and Clinical Outcomes
Primary, Double, and Triple Varus Knee Syndromes: Diagnosis, Osteotomy Techniques, and Clinical Outcomes
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


