Chapter 5 Normal and pathologic gait
Normal gait
Each limb blends the patterns of motion, passive force, and muscular control into a sequence of activity (called a gait cycle or a stride), which is repeated endlessly until the desired destination is reached. The two limbs perform in a reciprocal manner, offset by 50% of the gait cycle. The head, neck, trunk, and pelvis are self-contained passengers riding on the limb’s locomotor system.15
Basic functions
Progression
Functional phases of gait
Task I: Weight acceptance
Task II: Stance limb progression (single-limb support)
Task III: Swing limb advancement
Individual joint motion patterns
During stance, loading the heel initiates motion at each joint. Prompt response by the muscles provides an eccentric force that limits the arc of joint motion and also serves as a shock-absorbing mechanism. Recent investigations of eccentric muscle function, using portable ultrasound sensors (taped over the target muscle) have differentiated muscle fascicles from tendon during walking and jumping. These findings have redefined eccentric muscle action, which commonly is defined as a lengthening contraction. However, an ultrasound display of the muscle fascicles showed no increase in length.9 The gain in length was stretch of the tendon while the muscle exerted an isometric contraction to stabilize the joint; muscles only shorten or maintain neutral length.12
Ankle and foot
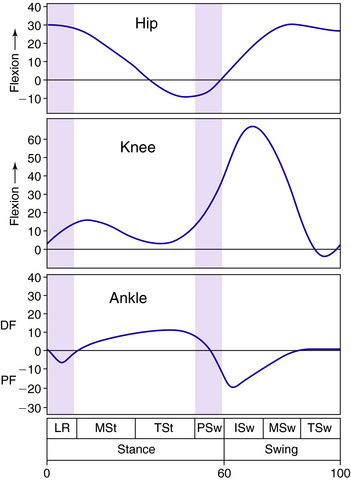
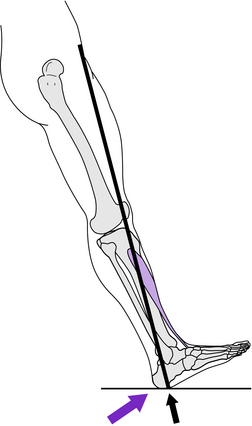
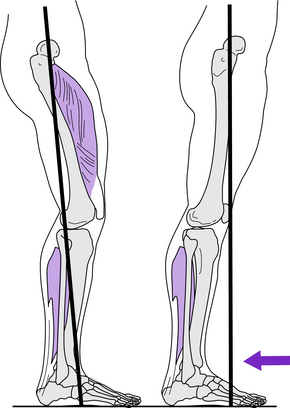
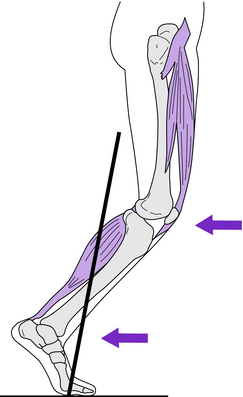
During each stride, the ankle passes through four arcs of motion (Fig. 5-1). At the onset of stance, the ankle is in neutral dorsiflexion, and floor contact is by the heel. Rapid loading of the heel causes the ankle to quickly plantar flex and then return to neutral before forefoot contact. Ultrasound analysis of muscle function at this time identified that the motion was the result of tibialis anterior tendon stretch.6 Release of the stretch force occurred as the heel lever shortened with the advancement of the vector across the heel. Following forefoot contact with the ground, ankle motion reverses to 10 degrees dorsiflexion as the tibia advances over the stationary foot for stance limb progression. Then the ankle plantar flexes 20 degrees during the final phase of stance (preswing). As toe-off starts swing, the foot again dorsiflexes under control of the pretibial muscles. Full elevation of the foot to neutral, however, is not completed until midswing.
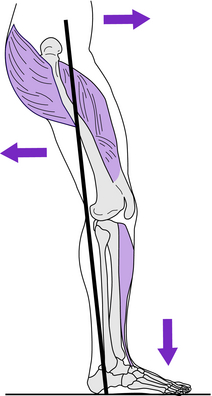
MP joint dorsiflexion is an essential component of heel rise. The foot rolls up over the base of the toes, particularly the great toe, as the trailing limb advances.14
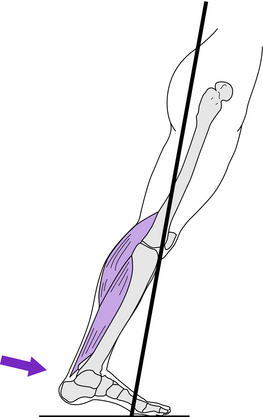
Dorsiflexion control is provided by the pretibial muscles (tibialis anterior, extensor hallucis longus, and extensor digitorum) during the loading response in addition to swing. The soleus and gastrocnemius control the tibia during stance limb progression. During terminal stance the EMG intensity of the gastrocnemius and soleus muscle mass increases rapidly in response to the dorsiflexion moment generated by the advancement of the body mass over the forefoot rocker. This same moment also stretches the tendon and gains 5 degrees of dorsiflexion at the ankle.9 In preswing, the tension of the Achilles tendon is abruptly released by the rapid transfer of body weight to the other limb. This creates a large power burst of plantar flexion by elastic recoil. The muscle mass is inactive (no EMG).9 The “push off” power generated is sufficient to initiate swing.12
Knee
Within each gait cycle, the knee alternately flexes and extends both in stance and in swing (see Fig. 5-1). From a position of full extension at initial contact, the knee rapidly flexes 18 degrees during weight acceptance. Ultrasound analysis shows this motion is the result of patellar tendon stretch while the quadriceps muscle is undergoing an isometric contraction.6 This is followed by progressive extension throughout the period of single stance, reaching a final position of 5 degrees flexion. The knee then rapidly flexes to 40 degrees during preswing and continues to 60 degrees in initial swing. From this position, the knee then extends to neutral.
Hip
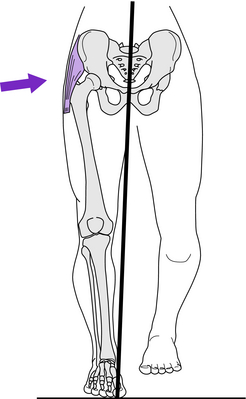
The major hip motions occur in the plane of progression (see Fig. 5-1). This consists of an arc of extension through stance, reaching 10 degrees hyperextension in terminal stance. A similar arc of flexion occurs from preswing through midswing. The resulting 35-degree flexed posture is maintained in terminal swing and loading response. In the other planes, there are small (4 to 5 degree) arcs of postural accommodation, which are described as pelvic motions.
Head and trunk
The basic function of the head and trunk is to maintain an upright posture. The small (5 degree) arcs of motion that occur reflect the uneven support provided by the reciprocal actions of the two limbs. Motion is greatest in the lumbar area and decreases at each higher segment. The spinal muscles act to preserve balance, absorb shock, and minimize head displacement.
Integrated function of the limb
Task I: Weight acceptance
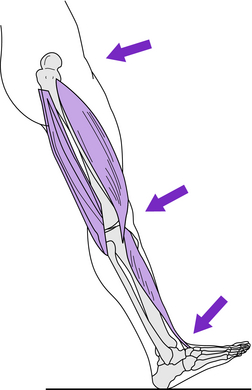
For both shock absorption and progression, the heel rocker drives the foot toward the floor as the limb is loaded. Response of the pretibial muscles to decelerate the dropping foot pulls the tibia forward. This places the vector behind the knee, leading to rapid knee flexion for shock absorption. Prompt quadriceps response opposes the vector’s flexor moment to preserve knee stability and absorb the shock of the initial floor impact. Knee extensor stability is aided by the femoral stability gained from the adductor magnus and gluteus maximus. Prompt relaxation of the hamstring muscles avoids an unnecessary flexor force.
Task II: Stance limb progression
Task III: Limb advancement






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


