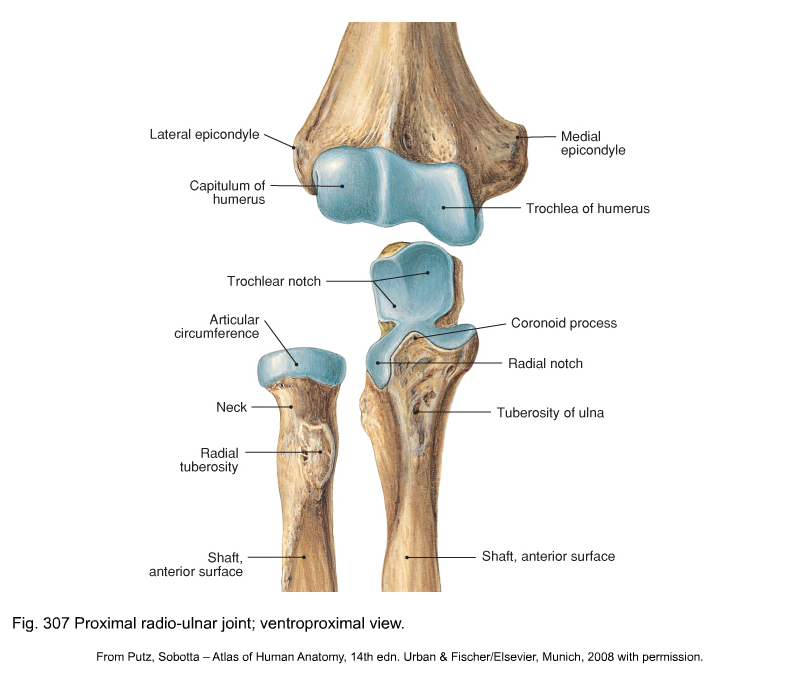
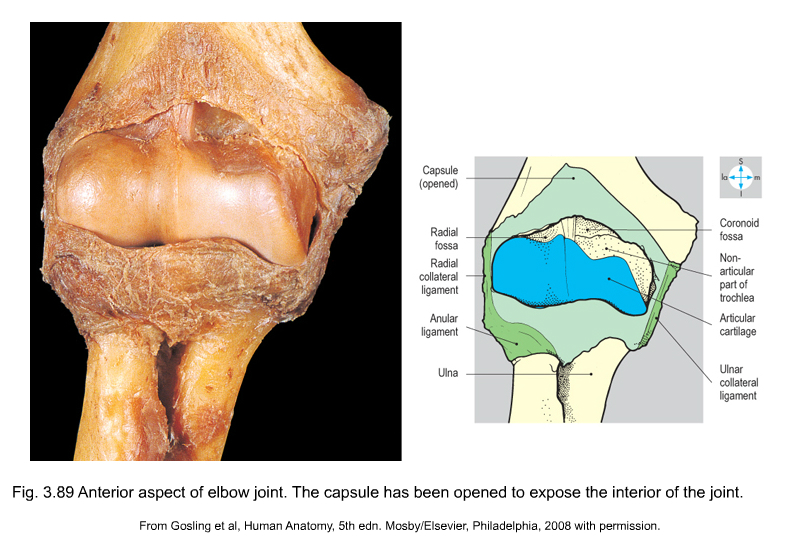
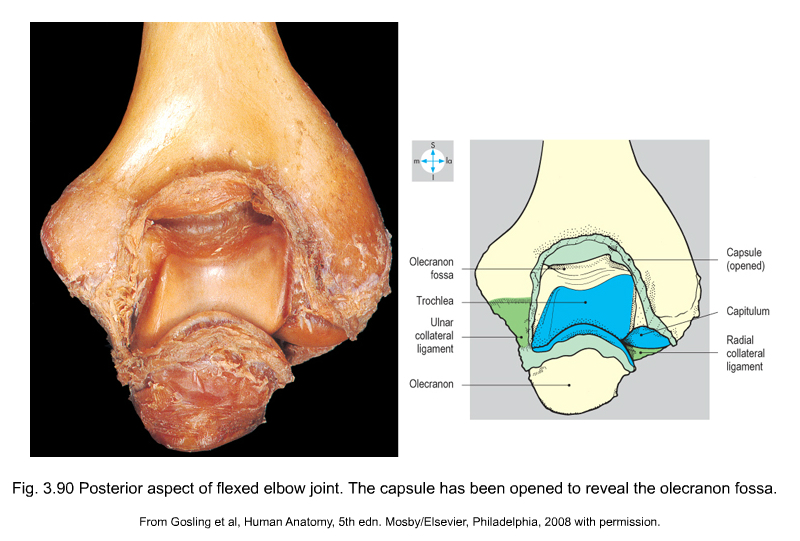
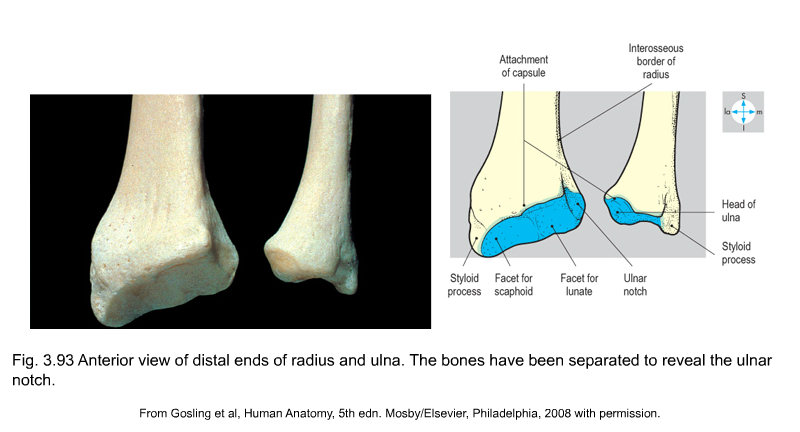
The three ‘joints’ are the humeroulnar, the humeroradial and upper radioulnar joint (Figs 1–3, see Putz, Fig. 307). Their two functions are flexion/extension, which is performed at the humeroulnar and humeroradial joints, and pronation/supination, which takes place at the upper radioulnar joint in close association with the lower radioulnar joint. • The humeroulnar joint acts as a hinge. The articular surfaces on the humerus are the spool-shaped trochlea with, proximal to it, the coronoid fossa (ventral aspect) (see Gosling et al, Fig. 3.89) and the olecranon fossa (dorsal aspect) (see Gosling et al, Fig. 3.90). The other part of the joint is formed by the olecranon, with its trochlear notch and its olecranon (proximal) and coronoid (distal) processes. • The humeroradial joint – a ball-and-socket joint – consists of (a) the spheroidal capitulum of the humerus and (b) the proximal surface of the head of the radius. Proximal to the capitulum lies the radial fossa and beside it a capitulotrochlear sulcus (between capitulum and trochlea). The articular facet of the radius, with which the proximal part of the humeroradial joint articulates, is at the top of the head of the radius. This facet exactly follows the shape of the humeral capitulum. Because it articulates with the capitulotrochlear sulcus at the ulnar side, it allows pronation–supination movements as well. • The upper radioulnar joint is a trochoid (cone-shaped) joint. The circumference of the head of the radius articulates with the radial notch of the ulna. The capsule is reinforced by strong lateral ligaments (Fig. 4): • The medial collateral ligament has an anterior part, which runs from the medial epicondyle of the humerus towards the annular ligament, a middle part towards the coronoid process, and a posterior part, directed towards the olecranon. All three parts are reinforced by an oblique band (ligament of Cooper) distally on the ulna. • The lateral collateral ligament connects the lateral epicondyle to the radial annular ligament (anteriorly via the radial collateral ligament and posteriorly via the lateral ulnar collateral ligament which inserts at the supinator crest of the ulna) and is interwoven with the superficial extensor muscles. • The radial annular ligament, a U-shaped fibrous collar, covered with cartilage at its inner aspect, joins the radial head to the proximal ulnar extremity so that they can articulate. It plays an important role in pronation–supination (see Gosling et al, Fig. 3.93). • The quadrate ligament attaches the radial neck to the distal aspect of the radial notch of the ulna. • The oblique cord extends inferolaterally from the lateral border of the tuberosity of the ulna to the radius, just below its tuberosity (see Putz, Fig. 315). It prevents downwards movement of the radius. • The interosseous membrane (see Putz, Fig. 315) and the oblique cord join the two bones of the forearm to prevent any longitudinal movement and assist as a fulcrum in pronation–supination (i.e. diagonal rotation). They are both syndesmosis connections. The trochlear surface of the humerus articulates with the trochlear notch of the ulna along an imaginary line A–A’ which runs slightly oblique (downwards and outwards) in its posterior course. This obliquity explains the physiological valgus position of the elbow in extension (Fig. 5). In its anterior course, the axis of movement is horizontal: therefore, in flexion, the forearm lies exactly in front of the upper arm. There are, of course, individual differences. Extension is mainly limited by the olecranon abutting against the posterior aspect of the humerus in the olecranon fossa (Fig. 6) and by stretching of the anterior part of the joint capsule. The forearm then usually lies in line with the upper arm, except in most women and in some men, in whom the elbow may sometimes overextend. This overextension is the result of the format of the olecranon fossa and process. The end-feel of this movement is hard.
Applied anatomy of the elbow

Joints and ligaments
Joints
Ligaments
Biomechanical aspects
Flexion–extension
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


anatomy of the elbow







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
