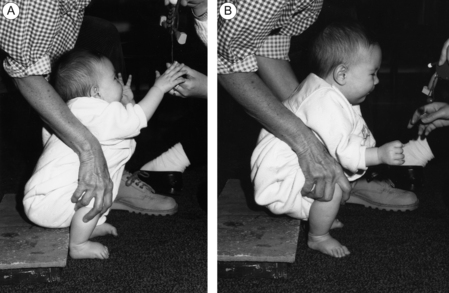
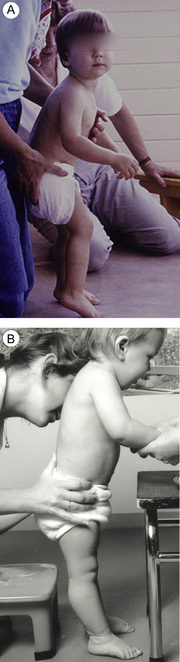
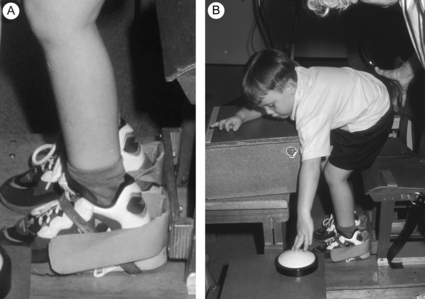
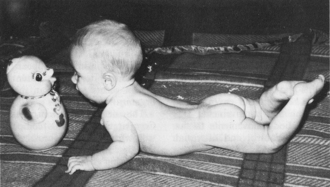
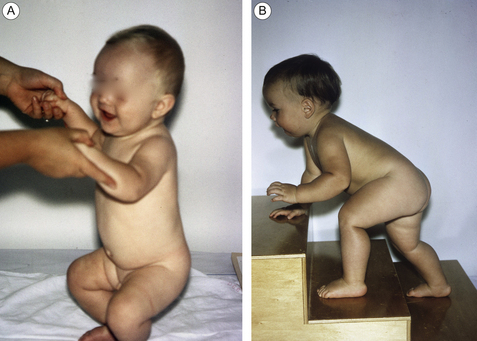
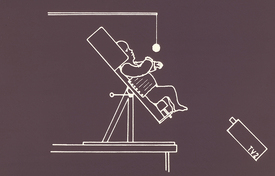
Annotation A Training and exercise for infants should focus on critical motor behaviours, those basic actions that are required for functional independence. In general, these actions comprise behaviours in sitting and standing that involve support, moving and balancing the body mass over the feet, e.g., actions such as squatting, sitting down and standing up (Fig. A.1), various forms of locomotion, and reaching out to grasp and manipulate objects. By working early in infancy to provide opportunities for repetitive practice of these basic actions, as occurs normally in the first year, one can expect some transfer or ‘generalizability’ into other actions that have similar underlying biomechanical characteristics as the infant explores the possibilities of the environment. Focusing on these basic actions early in infancy is likely to increase muscle activation and force production (strength) and preserve soft tissue flexibility and extensibility throughout the early period of bone and soft tissue growth. Modern concepts of motor development free us from the constraints of keeping within the boundaries of a sequential progression, e.g., rolling→sitting→crawling→standing→walking, proximal-to-distal. Figure A.1 Training a small infant to stand up and sit down. The therapist has placed the feet back and the infant is persuaded to stand up to take the toy, then sit down to put it on the floor, with repetitions and with reducing assistance. [From Shepherd RB 1995 Physiotherapy in Paediatrics 3rd ed. with permission from Elsevier.] The American College of Sports Medicine (2012) defines strength training as a systematic programme of exercises designed to increase an individual’s ability to exert or resist force. Strength is the capacity to produce the muscle forces necessary to carry out a particular action. It is relative to that action. Inherent in the word ‘strength’ is not only the amount and timing of force but also the ability to control it so that the muscles necessary to produce an action, that may involve one, two or more joints, work together co-operatively. Strength is a neuromuscular phenomenon, activity-specific and therefore functionally specific. Currently, there is increased interest in the importance of strength training in children and adults with brain lesions (American College of Sports Medicine et al., 2009), perhaps because of the long overdue recognition of the significance of poor muscle function and weakness as a major cause of functional disability. Muscle weakness is initially due to impairments affecting descending fibres to the spinal cord with decreased activation of motor units. However, weakness also occurs secondary to lack of physical activity imposed by the brain lesion and may eventually be more debilitating for the individual than the direct effects of the injury. It is possible that these secondary changes to the neuromuscular system may be preventable or reversible if active training starts in early infancy. This hypothesis has not been tested and there is a lack of investigation into strength (or muscle activation) in infants less than 18 months old with or without cerebral palsy (CP). Inadequate muscle activation (weakness) and poor motor control co-exist, and training should involve intensive active exercise both to strengthen muscles and to increase muscle control within the framework of a functional action. The strength required to perform basic motor actions is activity dependent (i.e., relative), and an able-bodied infant develops the necessary strength and control of the limbs during repetitive practice of a variety of novel actions. An infant normally finds many ways to practice moving the body mass about on the floor and over the feet in standing as part of the learning process (see Fig. 1.10). The activity-dependent strength of lower limb muscles gradually increases in response to practice of standing up from crouching and sitting, cruising sideways along the furniture, and in response to increasing load as the infant grows and body dimensions change. This vigorous and challenging practice may not occur for the infant with brain lesion unless it is planned. It is evident that we should be embarking on an exploration of ways to give young infants the early, intensive and varied practice they need but seldom get. Children with poor muscle function affecting lower limbs may not learn to bear weight and push down through the whole foot in standing up or in stance phase of walking, or to use the feet for balance and propulsion. This may, in part, be due to lack of experience in infancy of bearing weight through the feet in propulsive actions such as standing up and walking, and by the early development of calf muscle contracture (Fig. A.2A). Sitting with feet on the floor also needs to be practiced early to enable balance through the lower limbs while reaching in sitting and while standing up. The lower limbs play a significant role in balancing the body mass; hence the importance of ensuring sufficient active lengthening and force-generating ability of muscles that cross ankles, knees and hips and providing opportunities to develop appropriate foot alignment when weight-bearing. If this is not targeted early, over time small rearrangements of joints in the foot and abnormal growth of bones in the foot may make it impossible to distribute force appropriately over the plantar foot surface (Nsenga and Doutrellot, 2012), with negative effects on balance and lower limb alignment. Figure A.2 These two little boys with diplegia have not learned to take weight on their feet, flex forward at the hips, push their feet to the floor, and stand. (A) This boy has decreased extensibility of hip flexors and adductors, hamstrings, and calf muscles so he cannot extend his knees and hips or dorsiflex his ankles. (B) This boy has stiffened his legs; his ankles are not dorsiflexed so he will fall backward if not held. Exercises targeting these problems with training of functional lower limb actions are described in Chapter 11. [From Shepherd RB 1995 Physiotherapy in Paediatrics 3rd ed. with permission from Elsevier.] Actions that require weight-bearing through the plantar surface of the feet and propulsive force involved in pushing down through the feet may be critical to development of an appropriate relationship between plantar load receptors and motor control. Proprioceptive afferents from load detectors in the lower limb extensor muscles and ankle dorsiflexors (and perhaps the Golgi tendon organs) and exteroceptive afferents from mechanoreceptors in the plantar surface of the feet (plantar load receptors) appear to play a critical role in balance and walking (Dietz and Duysens, 2000). Extensor load receptors probably signal changes in the projection of the centre of body mass (CBM) with respect to the feet. Infants with diplegia or hemiplegia, for example, may persistently stand on the toes or fail to bear weight through the feet and push into the floor (Fig. A.2A,B). As part of training weight-bearing and balancing activities, crouching and standing up can be practiced using shoes attached to a flat surface as those shown in Figure A.3B. In this way the feet are held with heels on floor. Once the child gets the idea of pushing down through the feet, and flexing and extending hips, knees and ankles over the feet, he can practice without the shoes. Similarly, use of the upper limb for bearing weight and pushing into the support surface needs to be specifically targeted early in infancy (Figs A.4 and 1.3B, C). Figure A.3 (A) The shoe holder keeps the feet plantigrade while (B) the child practices squatting to press a light switch (one of the workstations in a circuit training class). The holder constrains the child’s foot so he cannot plantarflex and rise on to his toes. He can concentrate on flexing and extending his legs to increase strength and limb control. The exercise provides an active stretch to the calf muscles. Number of repetitions is monitored. i.e., he does as many as he can in the time allotted. Figure A.4 This normally developing infant shows a typical posture in prone, resting on the forearms, spine extended. The current view of strength training is that it must involve increasing repetition and increasing load (resistance). Carr and Shepherd (2010) provide an extensive review and discussion of issues related to strength training in adult neurorehabilitation, much of which is also relevant in paediatric practice. Below are some guidelines for strength training. The programme may need to continue throughout growth as movement control has to adapt to increasing height and weight. Damiano et al. (2002) have made a convincing case for muscle strengthening in children with CP. They have shown that these children have substantial and generalized muscle weakness that can contribute to bony deformity as well as motor dysfunction (Wiley and Damiano, 1998). Exercise principles for strength training are based on well-established scientific evidence and guidelines are readily available and modified for a disabled population and for children (American College of Sports Medicine et al., 2009; American College of Sports Medicine, 2012). Applying these principles to infant exercise is useful as a practical guide, but in practice some methods may be impractical until the infant reaches a certain stage. Exercise programmes must target specific goals, e.g., targeting strength, endurance or power training should lead to increased strength, or endurance, or power, but will not necessarily improve an individual’s cardiorespiratory endurance or energy cost unless the exercises are organized to stress aerobic capacity and efficiency (Damiano and Abel, 1998; Faigenbaum, 2000; Faigenbaum et al., 1999; MacPhail and Kramer, 1995). Older children are reported to have poor levels of fitness (Provost et al., 2007) and programmes should be developed to enable children with CP to be sufficiently and vigorously active to increase or maintain their fitness as they grow (Damiano, 2003), e.g., treadmill locomotion with or without harness, or water activities, or cycle ergometry. A small clinical study (Blundell et al., 2003) investigated the effects of lower limb strength training incorporated into task training in young children (aged 3−8 years) with diplegia, hemiplegia or quadriplegia. The children took part in a four-week group circuit training programme consisting of weight-bearing exercise designed to increase lower limb functional strength, balance through the feet, walking and sit-to-stand performance (Fig. A.5A–D). The exercises had similar biomechanical characteristics to many actions that involve the lower limbs in support, balance and propulsion. The exercises took into account the specificity principle in that muscle force generated was directly related to the functions being trained. Isometric muscle strength, performance of walking and sit-to-stand were significantly improved by the end of the programme and the effect was still present at the eight-week follow-up. Figure A.5 A circuit training class showing different workstations where children practice specific actions designed to increase lower limb strength and control. At each station the action can be made more challenging as the child improves. (A) Balancing with one leg in front of the other. He practices extending his left knee and hip with heel on ground, stepping back and forth with right leg while keeping the left hip extended. When he is ready he will take his hands off the table. In (B) both boys are trying to balance without using their hands for support. The boy on the right has soft splints to constrain his knees so he gets the ‘feel’ of weight-bearing without his knees collapsing; the boy on the left stops using the table for support when he is able. (C) Practice of crouch-to-stand and (D) stand ups from increasingly lower seats, keeping weight evenly distributed. This can be monitored by feedback from pressure-sensitive devices under each foot. Many other studies of children and adults with CP have found beneficial effects of strength training and several systematic reviews provide evidence that strength training can be effective (Bale and Strand 2008; Dodd et al., 2002, 2003; Liao et al., 2007; McBurney et al., 2003; Monkford and Coulton, 2008; Ryan et al., 2011; Taylor et al., 2005). What type of strength training is most effective depends on a number of factors, including the degree of weakness and a muscle’s strength relative to a specific action. In a recent study, 5–12-year-old children with mild diplegia (gross motor function classification system [GMFCS] 1 and 11) took part in a programme of loaded sit-to-stand (STS) resistance training, three times per week for six weeks. At the end of the programme their repetition maximum (RM) STS, scores on the Physical Cost Index, and gross motor function measure (GMFM) goal dimension score, were all significantly better than the control group. Interestingly, isometric (static) quadriceps strength and gait speed did not differ significantly from the control group, a result that supports the notion of specificity as the muscles were exercised isotonically (Liao et al., 2007). This study appears to be one of the first to specifically target the strength of an action, e.g., hip, knee and ankle extension and flexion (with feet on floor). It also targets the specific training of a major functional action instead of a complete physiotherapy programme, and therapists followed a set of guidelines, providing a good model for future studies of exercise effects. Although it is intuitive that a relationship between strength and function exists, we do not know what type of strength training has the best effects on functional performance and there appears to be no published investigations of infants under 12–18 months. From Buchner’s work with very weak adults (Buchner et al., 1996) it appears that, below a certain threshold of strength, exercise can result in some improvement in task performance (e.g., in walking). Above that threshold, however, function may not improve unless strength training is incorporated into skill training (e.g., increasing incline and speed in walking training and increasing load in STS training). Above a certain threshold, strength is task-dependent, i.e., the relative strength required for successful and stable performance of a particular action, such as, standing up from a seat, is not the same as absolute strength, the maximum load that can be lifted by the knee extensor muscles. One of the advantages of task-oriented exercise and training in young infants is that emphasis is not only on muscle activation and the production of muscle force but also on the control of that force, particularly the time it takes to build up peak force. Inability to generate force fast enough (lack of power) in lower limb muscles is probably a major factor underlying the inability to walk fast, run, jump and hop seen in children with CP, even in children who are independently mobile. Olney et al. (1991) have reported a positive correlation in adults with stroke between gait speed and the magnitude of push-off power* by the hemiparetic leg. The ability to time major power bursts is critical when walking, enabling, for example, increased speed, and a switch into running. Training, even for infants in the latter half of their first year, needs to incorporate variations in speed of movement and actions that require rapid force production for success (throwing, pushing, pulling, jumping, stair-climbing, increasing walking speed), i.e., exercises directed at power as well as strength. A major emphasis in infants should be on preserving the length and activation levels of calf muscles and hip and knee extensors for bearing weight through the feet in standing. These muscles can be exercised at the joint angle at which a major burst is required in specific functional actions; for example, as noted by Olney et al. (1988), muscles required for walking, concentric and eccentric ankle plantarflexion, can be exercised between about 10° dorsiflexion and 20° plantarflexion. Clinical studies in adults and children have failed to support the assumption that strengthening exercise might increase spasticity. Rather, strength training can result not only in increased muscle strength but also in improved functional motor performance, decreased resistance to passive movement and reductions in hyperreflexia (Bateman et al., 2001; Brown and Kautz, 1998; Damiano et al., 2001; Davies et al., 1996; Sharp and Brouwer, 1997; Teixeira-Salmela et al., 1999). Furthermore, strength training has positive effects on bone and muscle growth (Wilmshurst et al., 1996), and on muscle size and composition (Ryan et al., 2011). Children and adults with CP may have poor muscle endurance, a major factor in ambulatory decline and cessation (Bottos et al., 2001), and low levels of cardiorespiratory fitness (Damiano, 2003; Tobimatsu et al., 1998; Unnithan et al., 1998). The age at which a decline in cardiorespiratory fitness and of endurance is evident is not known in these children. However, it may start earlier than expected. The growing trend for training on treadmill (with harness support if necessary) and functional electrical stimulation (FES)-cycling machines, cycle ergometers and recumbent bicycles may help promote endurance training in children with CP, together with growing opportunities for exercise programmes and sporting activity (e.g., Provost et al., 2007; Ulrich et al., 2008; Unnithan et al., 2006). Some of these machines can be adapted for use by infants and small children, enabling them not only to increase control over their limbs but also to be vigorously active and to help them maintain or increase their fitness as they grow (see Figs 1.1 and 11.10 A–C). The force-producing capacity (tension regulation) of muscle differs according to whether the contraction is concentric or eccentric (Pinneger et al., 2000). Voluntary eccentric contractions produce greater force than concentric contractions yet involve lower rates of motor unit discharge than concentric contractions (Tax et al., 1990). In able-bodied adults, it has been shown that exercises involving concentric and eccentric contractions produce better gains in strength than exercises with concentric contractions alone. Figures 11.15–11.17 demonstrate exercises and activities for the lower limbs that involve switching between concentric and eccentric muscle contractions. When a muscle is actively stretched in an eccentric contraction, tension in the series elasticity component increases and the stored elastic energy is used in the subsequent concentric contraction (Svantessen and Sunnerhagen, 1997). Eccentric movements have to be practiced for skill in controlling such actions to be gained (Fig. A.3B). The effect of what is called the stretch-shortening cycle is seen when an eccentric contraction immediately precedes a concentric contraction, as in the brief flexion counter-movement seen in performance of the vertical jump. The concentric phase generates more force when it follows the flexion movement and the person jumps higher. A similar mechanism probably exists in walking (Komi, 1986) and in standing up (Shepherd and Gentile, 1994). The brief flexion at the knees in standing up, occurring at movement onset, provides a stretch to the knee extensor muscles, immediately prior to limb extension. In adult stroke patients, it is reported that a significantly larger concentric force occurred during limb loading in standing up after eccentric exercise on an isokinetic dynamometer (Engardt et al., 1995). From their research into changes in the mechanical properties of muscles in the affected limb after stroke, Svantessen et al. (2000) suggest that training activities in rehabilitation that emphasize eccentric–concentric exercise may result in more normal function and enhance recovery. It is evident that a major factor in developing skilled motor performance is training of the action itself and practice that is specific to the task and the different contexts in which it takes place (Magill, 2010). The infant needs verbal and visual guidance from a therapist/parent/sibling, who plans practice to ensure flexibility of performance in different environmental conditions. It has been an unspoken assumption in the neurofacilitation therapies that originated in the 1950s (e.g., Bobath’s neurodevelopment therapy) that movement facilitated by a therapist transfers or carries over to improved functional performance (Blauw-Hospers et al., 2007), but there is no evidence that this is so or that non-specific exercise will result in functional gain (Blauw-Hospers and Hadders-Algra, 2005). The body adapts specifically to the demands imposed upon it, for example, to the challenge to balance when we move our arms in standing. Whenever the therapist holds on to the infant as she/he tries to stand independently, the challenge to balance disappears and the infant cannot learn what must be done to move independently. Experiments have clearly shown that holding on to a support in standing changes the balance demands and therefore the pattern of muscle activation and joint movement (Fig. 11.4; Cordo and Nashner, 1982). Research over the years on the effects of motor training, including strength training in adults, has shown that exercise effects tend to be specific to task and context, i.e., what is practiced and where (Morrissey et al., 1995; Rutherford, 1988), with the greatest changes occurring in the training exercise itself. There is evidence, however, that transfer can occur between actions that share similar biomechanical characteristics (Buchner et al., 1996; Carr and Shepherd, 2003). The motor control system appears to use simplifying strategies. For example, the lower limbs are the focus in many activities that are performed while bearing weight through the feet. The basic pattern of intersegmental co-ordination is one of flexion and extension with the feet as a base of support (see Fig. 11.1). This pattern of co-ordination is seen in a number of actions significant to daily life that share major biomechanical characteristics, for example, standing up and sitting down, crouch-to-standing, stair ascent/descent (Fig. A.6A,B; see Chapter 11). Figure A.6 Flexion and extension at hips, knees and ankles form the basic pattern of intersegmental movement of lower limbs in many common actions. It is therefore possible that there can be some transfer from practice of one action to another. Two studies have exemplified this point: a study of children with CP by Liao et al. (2007) described earlier, and a study of adults after stroke by Dean and Shepherd (1997). In this study, seated subjects reached forward to grasp an object placed at the limit of reachability. The results showed that repetitive practice of various long-distance reaching tasks not only improved the distance that could be reached in sitting and the speed of reaching but also STS performance, yet STS had not been practiced. Perhaps it is not too surprising. The two actions share similar biomechanical characteristics in that both involve an initial horizontal momentum as body weight is shifted forward over the feet, with flexion at hips, knees and ankles. In training, subjects reached forward far beyond their arm length so that horizontal and vertical ground reaction forces generated through the lower limbs as the body moved forward would have been similar to those generated in the first phase of sitting to standing (Fig. 11.8B). The fact that speed of walking, unrelated to the action practiced, showed no change illustrates the significance of the specificity principle in exercise and training. Loss of tactile and pressure sensory discrimination also has major effects on the learning of manipulative tasks and dexterity. In precision grip during a grip and lift task, tactile information enables the adjustment of fingertip forces to the object’s weight and tendency to slip (Johansson and Westling, 1984; Westling and Johansson, 1984). The object’s texture is known to affect grip force, probably due to the perception of slippage (Cadoret and Smith, 1996). Johansson and Westling (1990) provided critical information for the training of object manipulation in their analyses of the role of tactile sensation in manipulation. It is clear that an infant’s early experiences should be organized to provide opportunities for the development of sensory discrimination along with motor performance. Singer (1982) noted that animal and human observations of vision suggest that experience-dependent maturation of sensory functions is set up by attentional mechanisms, and visual signals stimulate the development of normal receptive fields in the visual cortex of kittens only when the kittens are alert and attend to those signals. In terms of vision, the developing brain can screen incoming retinal signals and enable only selected patterns to alter cortical connections. Several decades ago, a series of interesting studies by von Hofsten (1982) showed that neonates can make extensive and complex arm movements. When they reached for a target they were more accurate when they looked at it than when they looked elsewhere. When von Hofsten videotaped newborns well-supported in a specially designed seat, he found that the arm was aimed closer to the target when the infants looked at it (Fig. A.7). By 2 months old, infants reached toward the target vigorously with arm extended and hand fisted; by 3 months, when looking at the object the infant opened the hand when reaching and the number of reaching attempts increased, apparently under visual control (von Hofsten, 1984). Figure A.7 The specially designed infant seat built for a reaching experiment. When training an infant in functional arm movements it is a good idea to follow the methods used in order to optimize performance in the experiment: the infant is well-supported, reaching to capture an attractive, graspable object that moves across the infant’s field of vision relatively close. [From von Hofsten C 1984 Developmental changes in the organization of pre-reaching movements. Develop Psychol 20:378–388, with permission from the American Psychological association].
Aspects of motor training
Targeted training and exercise
 Basic exercises to train step-ups, squats, push-ups, pulling, pushing, reaching
Basic exercises to train step-ups, squats, push-ups, pulling, pushing, reaching
 Task/activity-oriented exercises: standing up/sitting down, stepping/walking up and down stairs, reaching towards targets, reaching to manipulate, manipulating objects of different sizes, textures, for different purposes
Task/activity-oriented exercises: standing up/sitting down, stepping/walking up and down stairs, reaching towards targets, reaching to manipulate, manipulating objects of different sizes, textures, for different purposes
 Select actions that present a challenge to the infant: climbing a ladder, picking up a heavy object
Select actions that present a challenge to the infant: climbing a ladder, picking up a heavy object

Relationship between strength and function
Endurance and fitness
Concentric–eccentric muscle activity
Specificity and transfer
Specificity of sensory inputs
Related posts:
 B: Findings from a series of studies of passive mechanical properties of muscle in young children with cerebral palsy
B: Findings from a series of studies of passive mechanical properties of muscle in young children with cerebral palsy
 C: Kick start: using the mobile infant learning paradigm to promote early leg action
C: Kick start: using the mobile infant learning paradigm to promote early leg action
 Treadmill training in early infancy: sensory and motor effects
Treadmill training in early infancy: sensory and motor effects
 Very early upper limb interventions for infants with asymmetric brain lesions
Very early upper limb interventions for infants with asymmetric brain lesions
![]() Corticospinal tract development and activity-dependent plasticity
Corticospinal tract development and activity-dependent plasticity
 Training lower limb performance in early infancy: Support, balance and propulsion
Training lower limb performance in early infancy: Support, balance and propulsion
![]()
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


A: Aspects of motor training


