CHAPTER 1 Wrist Arthroscopy Portals
Introduction
Since its inception, wrist arthroscopy has continued to evolve. The initial emphasis on viewing the wrist from the dorsal aspect arose from the relative lack of neurovascular structures as well as the familiarity of most surgeons with dorsal approaches to the radiocarpal joint. Anatomical studies provided a better understanding of both the interosseous ligaments as well as carpal kinematics, which led to the development of midcarpal arthroscopy. Innovative surgeons continued to push the envelope through the development of techniques for treating intracarpal pathology, which in turn culminated in a plethora of new accessory portals. This chapter explores the standard arthroscopic portals, as well as some of the more recent and special-use portals.1
Indications
Midcarpal arthroscopy is essential in making the diagnosis of scapholunate and lunotriquetral instability. The grading scale reported by Geissler et al.2 provides a means of staging the degree of instability in order to provide an algorithm for treatment. Midcarpal arthroscopy is also useful for the assessment and treatment of chondral lesions of the proximal hamate.3 The triquetro-hamate joint can also be accessed through another special-use midcarpal portal.4
The clinical utility of volar portals has been recently elucidated.5–7 As kinematic and biomechanical studies have shed light on the role of the dorsal capsular structures and palmar subregions of the interosseous ligaments in maintaining carpal stability, it has become prudent to view the wrist from a palmar perspective. Volar portals for wrist arthroscopy have certain advantages over the standard dorsal portals for visualizing dorsal capsular structures as well as the palmar aspects of the carpal ligaments. The volar radial (VR) portal is relatively easy to use and is an ideal portal for evaluation of the dorsal radiocarpal ligament (DRCL) and the palmar subregion of the scapholunate interosseous ligament (SLIL). It facilitates the identification of and repair of DRCL tears.8,9 The VR portal also facilitates arthroscopic reduction of intra-articular fractures of the distal radius fractures by providing a clear view of the dorsal rim fragments.10
The volar radial midcarpal (VRM) portal may be considered an occasional accessory portal for visualizing the palmar aspects of the capitate and hamate in cases of avascular necrosis or osteochondral fractures.6 This portal facilitates visualization of the palmar aspect of the capitohamate interosseous ligament (CHIL), which is important in minimizing translational motion11 and has an essential role in providing stability to the transverse carpal arch.12
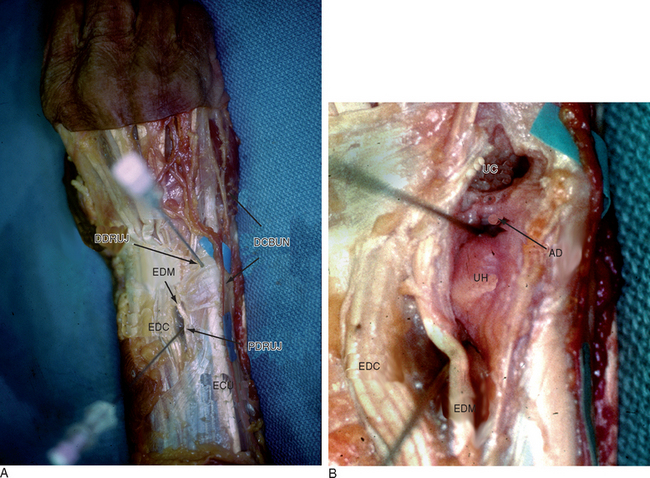
The volar ulnar (VU) portal provides unparalleled views of the dorsal radioulnar ligament and the dorsal ulnar wrist capsule, which contains the extensor carpi ulnaris subsheath (ECUS). Establishing the VU portal is more technically demanding but has potential use in the arthroscopic diagnosis and treatment of patients with ulnar sided wrist pain and suspected injuries to the ulnar sling mechanism. It is especially useful for visualizing and debriding palmar tears of the lunotriquetral ligament.13 It also aids in the repair or debridement of dorsally located TFC tears because the proximity of the 4/-,5 and 6R portals makes triangulation of the instruments difficult. The volar aspect of the distal radioulnar joint can be visualized through the VU portal to assess the foveal attachment of the triangular fibrocartilage in cases of suspected peripheral detachment of the TFC.7
Relevant Anatomy
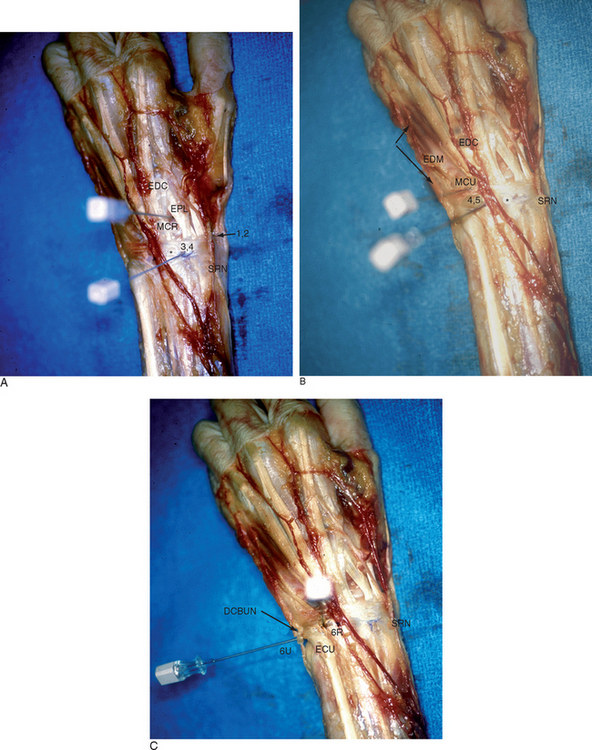
The standard portals for wrist arthroscopy are mostly dorsal (Figure 1.1a through c). This is in part due to the relative lack of neurovascular structures on the dorsum of the wrist as well as the initial emphasis on assessing the volar wrist ligaments. The dorsal portals, which allow access to the radiocarpal joint, are so named in relation to the tendons of the dorsal extensor compartments. For example, the 1-/,2 portal lies between the first extensor compartment tendons—which include the extensor pollicus brevis (EPB) and the abductor pollicus longus (APL)—and the second extensor compartment, which contains the extensor carpi radialis brevis and longus (ECRB/L).
Dorsal Cortals
Dorsal Radiocarpal Portals
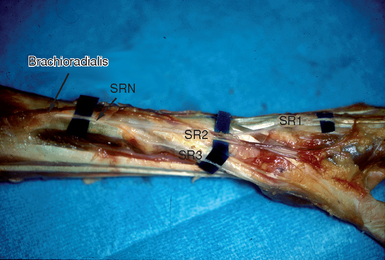
Abrams and co-workers performed anatomical dissections on 23 unembalmed fresh cadaver extremities and measured the distances between the standard dorsal portals and the contiguous neurovascular structures.14 The 1-/,2 portal was found to be the most perilous. The radial sensory nerve exits from under the brachioradialis approximately 5 cm proximal to the radial styloid and bifurcates into a major volar and a major dorsal branch at a mean distance of 4.2 cm proximal to the radial styloid15 (Figure 1.2). Branches of the superficial radial nerve (SRN) that were radial to the portal were within a mean of 3 mm (range 1 to 6 mm), whereas branches that were ulnar to the portal were at a mean of 5 mm (range 2 to 12 mm).
The radial artery was found at an average of 3 mm radial to the portal (range 1 to 5 mm). Either partial or complete overlap of the lateral antebrachial cutaneous nerve (LABCN) with the SRN occurs up to 75% of the time.16 In an anatomical study by Steinberg et al., the LACBN was present within the anatomical snuffbox in 9 of 20 (45%) specimens. Based on these findings, they recommended a more palmar, proximal portal in the snuffbox that was no more than 4.5 mm dorsal to the first extensor compartment and within 4.5 mm of the radial styloid.15
The dorsal cutaneous branch of the ulnar nerve (DCBUN) arises from the ulnar nerve an average of 6.4 cm (SD = 2.3 cm) proximal to the ulnar head and becomes subcutaneous 5 cm proximal to the pisiform. It crosses the ulnar snuffbox and gives off three to nine branches that supply the dorsoulnar aspect of the carpus, small finger, and ulnar ring finger.17 The mean distance of the dorsal cutaneous branch of the ulnar nerve (DCBUN) to the 6R portal was 8.2 mm (range 0 to 14 mm). Transverse branches of the DCBUN were found in 12 of 19 specimens and were noted to be within 2 mm of the portal (range 0 to 6 mm). The mean distance of branches of the dorsal cutaneous branch of the ulnar nerve (DCBUN) that were radial to the 6U portal was 4.5 mm (range 2 to 10 mm), whereas branches that were ulnar to the portal ranged from 1.9 to 4.8 mm on average. Any transverse branches of the DCBUN were generally proximal to the portal, at an average of 2.5 mm.
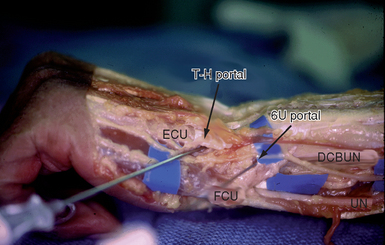
Triquetro-Hamate (TH) Portal
This portal enters the midcarpal joint at the level of the triquetro-hamate joint ulnar to the ECU tendon. The entry site is both ulnar and distal to the MCU. Branches of the DCBUN are most at risk (Figure 1.3).
Volar Portals
Volar Radial (VR) Portal
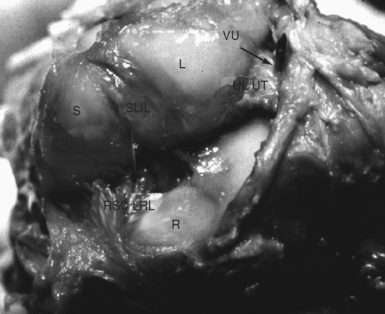
An anatomical study was performed on the arms of five fresh frozen cadavers to determine the safe landmarks for a volar radial (VR) portal after arterial injection studies to highlight the vascular anatomy.6 The proximal and distal wrist creases were marked. The volar skin was then removed and the flexor carpi radialis tendon (FCR) sheath was divided. The tendon was retracted ulnarly and a trochar was inserted into the radiocarpal joint at the level of the proximal wrist crease. The trochar was noted to enter the radiocarpal joint between the radioscaphocapitate ligament (RSC) and the long radiolunate ligament (LRL) in four specimens and through the LRL ligament in one specimen (Figure 1.5). The median nerve was 8 mm (range 6 to 10 mm) ulnar to the VR portal, whereas the palmar cutaneous branch passed 4 mm (range 3 to 5 mm) ulnar to the portal.
The radial artery was 5.8 mm (range 4 to 6 mm) radial to the portal and its superficial palmar branch was located 10.6 mm (range 6 to 16 mm) distal to the portal. The superficial radial nerve lay 15.6 mm (range 12 to 19 mm) radial to the portal. The portal was 12.8 mm (range 12 to 14 mm) distal to the border of the pronator quadratus, which roughly corresponds to the palmar radiocarpal arch.18 The palmar cutaneous branch was closest in proximity but always lies to the ulnar side of the FCR.19,20 The superficial palmar branch of the radial artery passed through the subcutaneous tissue over the tuberosity of the scaphoid and was out of harms way with an incision at the proximal wrist crease.21,22 When the trochar was placed through the floor of the FCR tendon sheath at the proximal palmar crease, the carpal canal was not violated. It was thus apparent that there was a safe zone comprising the width of the FCR tendon and at least 3 mm or more in all directions. This zone was free of any neurovascular structures.
Volar Radial Midcarpal (VRM) Portal
The volar aspect of the midcarpal joint was identified with a 22-gauge needle through the same skin incision and a blunt trochar was inserted. It was necessary to angle the trochar in a distal and ulnar direction (approximately 5 degrees) in order to access the midcarpal joint through the same skin incision. The trochar passed closer to (but still deep to) the superficial palmar branch of the radial artery, which coursed more superficially over the scaphoid tuberosity at that level. The distance between the volar radiocarpal and volar midcarpal entry sites averaged 11 mm (range 7 to 12 mm).
Volar Ulnar (VU) Portal
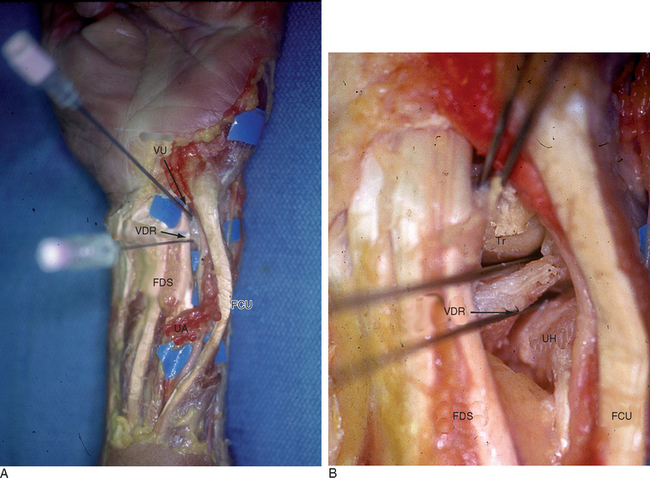
In a companion study, a volar ulnar (VU) portal was established via a 2-cm longitudinal incision made along the ulnar edge of the finger flexor tendons at the proximal wrist crease.13 The flexor tendons were retracted radially and a trochar was introduced into the radiocarpal joint. The ulnar styloid marked the proximal point of the VU portal, approximately 2 cm distal to the pronator quadratus. The portal was in the same sagittal plane as the ECU subsheath and penetrated the ulnolunate ligament (ULL) adjacent to the radial insertion of the triangular fibrocartilage. The ulnar nerve and artery were generally more than 5 mm from the trochar, provided the capsular entry point was deep to the ulnar edge of the profundus tendons.
The palmar cutaneous branch of the ulnar nerve (nerve of Henlé) was highly variable and not present in every specimen. This inconstant branch provides sensory fibers to the skin in the distal ulnar and volar part of the forearm to a level 3 cm distal to the wrist crease. Its territory may extend radially beyond the palmaris longus tendon.23 This branch tends to lie just to the ulnar side of the axis of the fourth ray, but it was absent in 43% of specimens in one study.24 Martin et al. demonstrated that there was no true internervous plane due to the presence of multiple ulnar-based cutaneous nerves to the palm, which puts them at risk with any ulnar incision.19 Because there is no true safe zone, careful dissection and wound spread technique should be observed.
Field of View
The following sections describe the typical field of view as seen through a 2.7-mm arthroscope under ideal conditions.25,26 Synovitis, fractures, ligament tears, and a tight wrist joint may limit the field of view (which necessitates the use of more portals to adequately assess the entire wrist).
1-/,2 Portal
Structures visualized are limited to the radial half of the wrist.
3-/,4 Portal
This is almost a complete panoramic view of the entire volar radiocarpal joint.
< div class='tao-gold-member'>
Related posts:
 Arthroscopy of the Distal Radioulnar Joint
Arthroscopy of the Distal Radioulnar Joint
 Arthroscopic Plication of Lunotriquetral Ligament Tears
Arthroscopic Plication of Lunotriquetral Ligament Tears
 Arthroscopic Treatment of Scapholunate Ligament Tears
Arthroscopic Treatment of Scapholunate Ligament Tears
 Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
Arthroscopic Debridement for Isolated Scaphotrapeziotrapezoid Arthritis
 Arthroscopically Assisted Reduction and Percutaneous Fixation of Scaphoid Fractures Using a Simple External Targeting System
Arthroscopically Assisted Reduction and Percutaneous Fixation of Scaphoid Fractures Using a Simple External Targeting System
 Peripheral Tears of the TFCC: Arthroscopic Diagnosis and Management
Peripheral Tears of the TFCC: Arthroscopic Diagnosis and Management
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


