CHAPTER 4 WRIST AND HAND
A LIGAMENT/INSTABILITY TESTS
Piano key test
Clinical context
Isolated involvement of the IRUJ is rare and is usually associated with more significant injury at the wrist (i.e. fracture or dislocation). Minor disruption may cause pain as the primary sign and this would be well localized with tenderness easily elicited by palpation (see clinical tip). Pain at the end of passive pronation and supination would also be provocative. Where ligament disruption has occurred, excess movement will be accompanied by apprehension during certain activities, particularly in weight-bearing positions where its lack of stability is more seriously tested.

The IRUJ is often involved in inflammatory arthritis and in more severe cases, the synovitis afflicting the joint causes a destructive process resulting in pronounced loss of rotation, dorsal prominence and instability of the ulna, as well as localized swelling and loss of the normal function of the adjacent extensor carpi ulnaris, a condition known as caput ulnae syndrome (Brown & Neumann 2004). Given the associated joint stiffness, despite the instability at the IRUJ, the piano key test may not yield a positive result.
Clinical tip
| EXPERT OPINION | COMMENTS |
|---|---|
 | Piano key test |
| Especially useful to determine level of instability – only a very unstable joint will behave like a true ‘piano key’. |
Radial collateral ligament stress test

Clinical context
This test is most likely to identify an isolated sprain of the RCL where localized pain around the anatomical snuffbox would be the primary complaint. Depending on the severity of the trauma, a varying but equal degree of flexion/extension restriction may also be present at the wrist as the ligament blends with, and reinforces, the lateral joint capsule, thereby causing capsular limitation. As the history is usually traumatic, careful screening is necessary (including X-ray evaluation in most cases) to eliminate fracture of the carpus – the scaphoid being the usual culprit. With pain reported in this area, osteoarthritis of the trapeziofirstmetacarpal joint (basal joint of the thumb; see axial compression test, p. 129) and de Quervain’s tenosynovitis (see Finkelstein’s test, p. 131) are other possible diagnoses to consider.
Clinical tip
| EXPERT OPINION | COMMENTS |
|---|---|
 | Radial collateral ligament stress test |
| Usually included as part of radiocarpal assessment without specifically testing the ligaments as they are rarely injured in isolation. |
Ulnar collateral ligament stress test

Clinical tip
The ligament is most easily identified by finding the styloid with the wrist in ulnar deviation and then passively moving the wrist radially until the ligament can be felt tautening under the finger.
| EXPERT OPINION | COMMENTS |
|---|---|
 | Ulnar collateral ligament stress test |
| Usually included as part of radiocarpal assessment without specifically testing the ligaments as they are rarely injured in isolation. |
Scaphoid shift test
Technique
Action
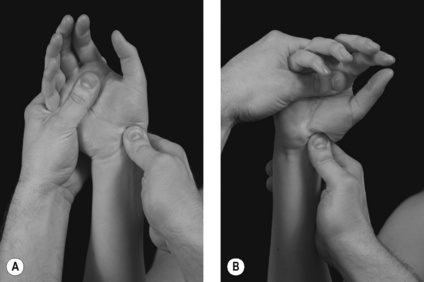
Firm pressure is applied on the scaphoid while the hand is taken initially into ulnar deviation and slight extension to offload the scapholunate articulation (Fig. 4.4A). Maintaining the pressure on the scaphoid, the wrist is then taken slowly into radial deviation and slight flexion creating a subluxation force that stresses the articulation and exposes instability if present (Fig. 4.4B).
Positive test
Excessive movement of the scaphoid in relation to the lunate is detected along with some pain and/or apprehension. If subluxation occurs the proximal pole of the scaphoid shifts dorsally over the dorsal rim of the radius. Removing the pressure from the palmar aspect of the scaphoid and returning the wrist into some ulnar deviation and extension will cause the scaphoid to shift back in a palmar direction to its reduced, normal position.
Clinical context
Although comparatively rare, the instability that results from disruption of the scapholunate articulation is the most common carpal instability. A complete tear of the scapholunate ligaments, usually resulting from a severe hyperextension injury, will lead to significant scapholunate dissociation and disruption to the normal motion of the proximal carpal bones during wrist movement. Because of the loss of connection between the scaphoid and lunate, the scaphoid rotates into a degree of flexion leaving the lunate and triquetral free to rotate into extension which causes pain, an inability to weight-bear on the wrist and an overall loss of function (Placzek & Boyce 2006). Chronic instability of the joint also strongly predisposes to a recognized sequence of osteoarthritis involving the unstable capitolunate and capitoscaphoid articulations (particularly in the presence of a dorsally subluxed capitate) and, more latterly, the radioscaphoid and radiolunate joints, a sequence known as scapholunate advance collapse (SLAC) (Miller & Schweitzer 2005).
The normal extent of separation between the scaphoid and lunate bones should be less than 2 mm (Gross et al 2002) but a diastasis of more than 3 mm is pathognomonic of scapholunate dissociation and should be detectable on plain X-rays (McRae 1990). The evident space between the bones is known as the Terry Thomas sign, named after the 1960s comedian who famously had a gap between his two front teeth (Placzek & Boyce 2006).
Using a cadaver model where the wrist was progressively loaded in extension and ulnar deviation (the most common mechanism of injury), a sequential, four-staged pattern of injury was noted; scapholunate diastasis, dorsal subluxation of the capitate, disruption of the lunotriquetral ligament and complete dislocation of the scapholunate articulation (Brown & Neumann 2004). Subluxation of the capitate (see clinical tip) is therefore usually associated with injury to the proximal carpus although it does not have to involve catastrophic disruption of the scapholunate articulation (see capitate apprehension test, p. 124).
Clinical tip
Care should be taken when interpreting the findings as up to 30% of healthy wrists can give a false positive result due to general ligamentous laxity at the wrist. It is thought that repeating this dynamically (see variations), particularly when the patient makes a fist, reduces this tendency (Weiss & Finkelstein 2005).
| EXPERT OPINION | COMMENTS |
|---|---|
 | Scaphoid shift test |
| A tricky test to perform, as well as interpret, but very useful once perfected. |
Lunotriquetral shear test
Technique
Patient position
The patient is seated with the forearm supinated and comfortably supported on a table.

Clinical context
Differing descriptions for this test can be found in the literature and this has led to the same test being assigned several names. Injury to the lunotriquetral articulation is uncommonly encountered (see scaphoid shift test, p. 119) requiring impact in extension and radial deviation (Brown & Neumann 2004). A strain to the lunotriquetral ligament may be evident with localized tenderness and a positive test, but if the trauma has been sufficiently significant to cause disruption of the articulation, normal kinematics will be lost. The combined unit of the scaphoid and lunate rotate into flexion leaving the untethered triquetral to drift into extension. Pain, apprehension, a reluctance to move and weakness will all be reported by the patient, with a more significant injury likely to predispose to osteoarthritis (Placzek & Boyce 2006). Lunotriquetral ligament injury is often associated with triangular fibrocartilage complex (TFCC) tears (see TFCC test, p. 127) and MRI can therefore be helpful in making the distinction (Miller & Schweitzer 2005). There are no studies examining the reliability of this test and considerable skill is required to interpret the findings meaningfully.
Clinical tip
An isolated injury to the lunotriquetral ligament does not usually produce a static diastasis between the lunate and triquetral so there may be dynamic and functional instability present but a normal plain X-ray reported.
| EXPERT OPINION | COMMENTS |
|---|---|
 | Lunotriquetral shear test |
| It is important to establish what is normal excursion on the unaffected side as differences in range can be subtle. |
Capitate apprehension test








