Early Weightbearing of the Lapidus Bunionectomy
Is it Feasible?
Keywords
• Lapidus bunionectomy • Early weightbearing • Nonunion • Fusion
The Lapidus procedure is no longer considered a strict nonweightbearing bunionectomy.1–12 Rigid internal fixation has provided stability of the fusion construct, allowing surgeons to mobilize patients sooner than traditionally thought.2,3 Studies have emerged demonstrating that early weightbearing programs achieve fusion rates equivalent or better than nonweightbearing protocols.1,4–9 The orthopedic industry has also recognized this shift and produced specialized plating systems to provide additional and alternative fixation options.
What is a Lapidus bunionectomy early weightbearing program?
Time to Initiate Early Weightbearing Protocol
Some recommend a period of nonweightbearing for 2 weeks after the surgery to allow for soft tissue healing.1 Others allow immediate weightbearing as tolerated.6 Nonetheless, each surgeon has their own protocols based on their experiences and comfort level. As surgeons continue to use early weightbearing programs and have satisfactory results, protocols continue to advance.
Type of Extrinsic Protection
The fusion site still needs to be supported extrinsically during the postoperative healing process. Surgeons have used weightbearing short leg casts, removable walking boots, and postoperative shoes. A cast provides the most amount of protection.10 A removable boot allows for patients to specifically exercise the foot and ankle. A postoperative shoe provides the least extrinsic support, and surgeons should be confident that the internal fixation is stable enough to support the loads of weightbearing when choosing this method.
Amount of Weight Allowance
The amount of weight that a patient can place postoperatively is also not clearly delineated. Some advocate gradual increases in weightbearing pressure over the course of 6 weeks, whereas others allow immediate weightbearing. Proper patient selection and fixation method are probably the most critical factors when selecting patients suitable for a postoperative weightbearing program after Lapidus bunionectomy.1,2
The stigma of nonunion with postoperative weightbearing
Early experience with the Lapidus procedure resulted in a nonunion rate up to 25%, and this was a major deterrent to surgeons performing the Lapidus procedure.3 Postoperative weightbearing was inappropriately blamed as the cause of the nonunions, and it was not until experience with the Lapidus that poor inadequate nonrigid fixation was demonstrated to be the cause of the high nonunions seen in the early part of the century.
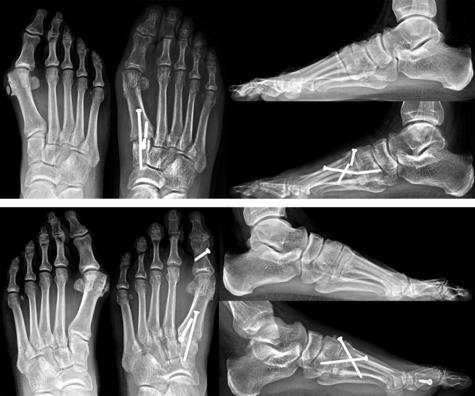
Dr Paul Lapidus also experienced this high nonunion rate (in the 1930s) because the fixation method of choice was suture.13–15 Screw fixation was introduced in the 1970s and surgeons started performing the procedure with more regularity in the 1980s.10,11,16 Screw fixation provided stability of the fusion, allowing for more reliable and acceptable fusion rates (Figs. 1 and 2).


Experience and better fixation methods have brought the nonunion rate to 3% to 12% of cases, a more palatable number for surgeons.17–24 Recent studies have suggested that the nonunion rate is even lower in 0% to 5.3% of cases.1,25 Nonunions exists even in the best hands and for the most part should not be considered a complication, but rather an expected outcome in a low percentage of cases.
There are patient and surgeon factors that can contribute to nonunion occurrence. Surgeons should be mindful of the technical aspects of the procedure and chose a stable fixation method to decrease the possibility of nonunion. Nonetheless, some patients are predisposed to bone healing difficulties because of genetic factors, medical comorbidities, and habits (ie, smoking) (Fig. 3). Furthermore, nonunions may be asymptomatic (not painful) and should be considered a radiographic finding.
Literature and early weightbearing Lapidus
Although early weightbearing seems like a new concept, it is not. Lapidus’s postoperative protocol was weightbearing in postoperative shoe with a medial plate.13–15 Fixation options were limited at that time to support early weightbearing. However, because rigid internal fixation was introduced in the late 1980s for Lapidus arthrodesis there have been numerous studies demonstrating that early weightbearing is an acceptable postoperative protocol.1,4–12 Between 1987 and 1992, only four studies regarding early weightbearing were produced. There was a lag of 17 years before the next wave of publications emerged and surgeons became comfortable with the procedure and improved techniques. Between 1992 and the present, seven publications demonstrate a variety of postoperative early weightbearing protocols with satisfactory results.
Sangeorzan and Hansen10 retrospectively reviewed Lapidus procedures with crossed screw fixation and an early weightbearing program in 40 feet. Their protocol involved immediate toe touch weightbearing in a short leg cast for 2 weeks. Patients were then allowed “weight of leg ambulation” for an additional 2 weeks in the cast, then full weightbearing for an additional 4 weeks until radiographic evidence of union was identified. Radiographic union was achieved in 92%. Three patients underwent revision for nonunion. Using the same postoperative early weightbearing protocol discussed previously, Clark and coworkers11 evaluated the Lapidus arthrodesis in an adolescent population (average age of 18) in 32 feet. Fusion rate was 100%.
Bednarz and Manoli26 performed a consecutive review of 31 feet after Lapidus arthrodeses with screw fixation. A 100% union rate was seen in their early weightbearing protocol. Patients were nonweightbearing for 2 weeks followed by protected weightbearing for 2 to 6 weeks.
Myerson and colleagues12 evaluated 67 feet after a first metatarsocuneiform joint fusion. Twenty-one feet were placed in a short leg cast and crutches until comfortable weightbearing was tolerated. The remaining 46 feet were ambulating in a postoperative shoe with or without crutches for a duration of 6 to 8 weeks. There were seven radiographic nonunions (9.5%) and only one patient underwent a revision fusion.
Sorensen and coworkers8 retrospectively reviewed locking plate fixation and early weightbearing. Fusion rate was 100%, and the average time to radiographic fusion was 6.95 weeks with an average time to ambulation of 2 weeks.
Kazzaz and Singh7 allowed postoperative weightbearing in a postoperative shoe in 27 feet and achieved a successful fusion in 6 to 24 weeks, in a retrospective review. The authors attributed the success to modern techniques of minimal bone resection, meticulous bone surface preparation, and rigid internal fixation.
Saxena and coworkers9 performed a retrospective comparison of outcomes of Lapidus following cross screw fixation versus locking plate with screw fixation in 40 patients. The locking plate group was allowed full weightbearing at 4 weeks, whereas the screw fixation group was allowed at 6 weeks. There were no differences in postoperative complications between the two groups, and the locking plate Lapidus allowed for earlier weightbearing.
Basile and colleagues6 retrospectively reviewed immediate weightbearing after modified Lapidus arthrodesis when two screws and a neutralization K-wire fixation were performed in 41 patients. They compared an early weightbearing protocol (immediate partial weightbearing in a removable boot) with a nonweightbearing protocol (short leg cast for 6 weeks postoperatively). No nonunions were identified and the authors suggested that a “third point of fixation may enable immediate protected weight bearing, by minimizing load placed on the crossed lag screw construct, in patients undergoing modified Lapidus arthrodesis.”
In a multicenter review of 80 feet, Blitz and colleagues1 retrospectively reviewed an early weightbearing protocol with screw fixation (two to three screws). All patients were allowed protected weightbearing after the first postoperative visit. All 80 feet proceeded to successful union (100% union), and the mean time to union was 44.5 days. Patients began protected weightbearing at a mean 14.8 days postoperative.
DeVries and colleagues5 performed a retrospective comparison of screw fixation versus plate fixation in 143 Lapidus tarsometatarsal (TMT) joint arthrodesis. Time to full weightbearing and union rate demonstrated statistically significant improvement (P<.001) when locking plates were used. Locking plate and early weightbearing demonstrated a 98.5% union rate.
Menke and colleagues4 retrospectively reviewed an early weightbearing program in 21 Lapidus fusions with locking plate combined with a single interpositional screw. Successful fusion was achieved in 90.5% and the mean time to weightbearing was 4.7 weeks.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


