, Paul D. Siney1 and Patricia A. Fleming1
(1)
The John Charnley Research Institute Wrightington Hospital, Wigan, Lancashire, UK
Charnley was probably the first to suggest that “late failure … may be expected from tissue reaction to particles abraded from the bearing surfaces”.
Pain relief is the hallmark of a successful total hip arthroplasty; the natural symptomatic joint is replaced with an artificial, neuropathic spacer functioning within a foreign body bursa.
Activity level achieved after the operation is not a characteristic of a particular design nor the method of component fixation, provided it remains secure when under load, it is a reflection of patient selection for the operation.
This method of surgery demands not only the clinical skill of patient selection but also the practical skill of component fixation. That skill will be tested severely by the repeated loading of the implant within the ever changing skeleton.
The consequences of improved function can be expressed as load and sliding distance at the articulation and quantified as wear.
Wear has two basic elements: wear products shed into the tissues and structural changes of the articulation.
We are concerned here with wear of the UHMWPE cup and its effect on component fixation.
Since absolute rigidity does not exist in nature, the quality of component fixation, in the context of the neuropathic spacer, total hip arthroplasty, cannot be defined in terms that may be acceptable to all. By analogy failure of fixation cannot be defined in terms of clinical results. Hence, clinical results cannot be expected to reflect the mechanical state of the arthroplasty: the quality of component fixation.
The role of UHMWPE wear particles, the tissue reaction they stimulate and the possible effects on component fixation, continues to be of wide interest.
It was Willert and Semlitsch [1] who were quite definite in their conclusions derived from the studies of hip endoprosthesis: cobalt chromium alloy articulating with polyethylene or polyethylene terephthalate. They stated that granulation tissue may act on the neighbouring bone “which is removed by extensive resorption leading to loosening of the prosthesis”.
With an increasing number of publications the terminology changed: “cement disease” gave way to “cementless disease”, “particle disease”, “poly disease” and “access disease” as the causes of component loosening we proposed.
Eventually “osteolysis” became and continues to be the term used to define not only the effects of tissue reaction to wear particles, but also the cause of component loosening.
What has happened, almost certainly inadvertently, is that radiographic appearances at the bone-cement interface – were ascribed as being due to a definite pathological process- osteolysis – removal of calcium of bone and was now responsible for component loosening.
It is that leap of reasoning: from tissue reaction to UHMWPE wear particles, a very definite entity, to loosening of components, a very definite mode of failure, without consideration of the mechanical causes of failure, that has resulted in a number of changes in materials, design and methods of component fixation.
Study of alternative materials is essential but must be planned with caution and in the full knowledge of past experience. Comparable follow-up is essential.
Attempts at counteracting tissue response to UHMWPE wear particles is unlikely to be of long term value. It is unlikely that the human body will respond specifically to a particular implant material, provided its chemical state, immunological response or mutation potential has not been affected. To argue otherwise would be to accept the unlimited possibilities of response to the vast ingenuity of the inventor and designer. As for the technique of component fixation: “Surgeons yearn for an easy hip operation” finds a response in “cementless” implants which aim to replace the technical skill, a commodity that cannot be sold at a profit, with an implant which becomes a profitable product.
It is essential that the mechanical environment of the foreign body bursa – the total hip arthroplasty – be examined for any possible improvements before attempting wholesale changes based on incomplete evidence.
Wear of UHMWPE Cup: Mechanical Consequences
Nowhere in the locomotor system would liaison with university departments of engineering and colleges of technology be more rewarding than in the biomechanics of the hip joint.
Changes in geometry resulting from wear are easily understood and can be reproduced and tested experimentally. It is here that collaboration with scientific institutions and industry is invaluable.
Charnley commented on this aspect half a century ago: Basic mechanical changes resulting from wear will be discussed briefly – Friction characteristics, frictional torque, decreasing rigidity of the cup wall, impingement, external cup wear and finally the incidence of cup loosening in relation to cup penetration. It must be accepted that the changes are inter-related and all contribute to cup loosening.
Changes in Friction Characteristics
Hall et al. (1994) [2] studied 54 explanted and 5 new Charnley hip prostheses. Frictional resistance was measured using the Durham hip function simulators both under dry and lubricated conditions.
The friction factor for the new prostheses showed normal, bell-shaped scatter. This distribution was skewed for the explanted prostheses; although most retained comparable friction values, a significant number showed increased frictional resistance. Friction factor did not increase with the depth of cup penetration or follow-up. There was no clear correlation between friction factor and whether the cups revised were loose or exchanged for other reasons. The conclusion was that increased friction alone is unlikely to be responsible for the increasing rate of cup loosening observed with increasing depth of cup penetration.
Decreasing Rigidity of the Cup Wall
Increasing depth of cup penetration reduces the thickness of the cup wall increasing the amplitude of deflection under load. This aspect has not been a subject of detailed studies. Its clinical significance is not easy to establish. Careful examination of serial radiographs may reveal the evidence: fracture of the wire marker in the region of the direction of cup wear with fracture of the acetabular cement, (Fig. 36.1) localised cavitation around cement peg (Fig. 36.2) and wear-out and fracture of the cup without cup loosening (Fig. 36.3) [3].


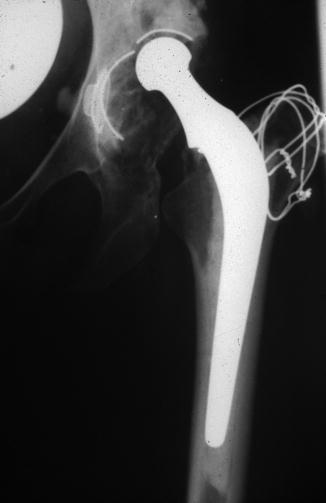
Fig. 36.1
Fracture of the wire marker in the region of the direction of cup wear with fracture of the acetabular cement
Fig. 36.2
Wear of the cup and localised cavitation around cement peg
Fig. 36.3
Wear and fracture of the UHMWPE cup. (Note the cup is not loose – medially)
Impingement
Charnley et al. [4] were the first to suggest that more than 5 mm wear might cause impingement of the neck of the prosthesis against the inner rim of the cup and cause loosening at the bone-cement interface. Pursuing the concept of impingement Hall et al. [5] examined 74 explanted Charnley cups.
A strong positive association was observed between penetration depth and impingement irrespective of whether the neck diameter was 12.5 mm or 10 mm.
Reducing the diameter of the neck of the stem from 12.5 to 10 mm reduced the probability of impingement.
With the 12.5 mm diameter neck there was 50 % probability of impingement at zero penetration.
With the 10 mm diameter neck the 50 % probability of impingement did not occur until 2 mm of cup penetration had been reached.
The conclusion was: “if impingement is a problem then the reduced diameter neck appears to be a solution in cutting rates of long-term cup loosening”[5].
External Cup Wear [6, 7]
Examination of 159 explanted cups showed areas of wear on the outer surface. It was found in 53 (33 %) of cups. Their size increased with follow-up and depth of cup wear. Appearances indicate a ‘to and fro’ rocking movement against the acetabular bone – a mechanical cause.
Depth of Cup Penetration and Incidence of Cup Loosening
Studies on the subject of cup wear (penetration) and loosening are summarised.
Patients under the age of 40 at surgery (1984). Seventy one patients; 104 LFAs, mean age of 32 years at LFA and a follow-up of 9.3 years (4–17) showed increasing incidence of cup migration with increasing depth of cup penetration (Table 36.1, Fig. 36.4) [8].
Table 36.1




Details of 1984 study. Correlation between depth of cup penetration (mm) and the incidence of cup migration (%)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree
