Abstract
Objectives
To establish the level of maximal aerobic capacity in patients with chronic pain of different etiologies and to compare these results with different parameters of disability.
Patients and methods
A cycloergometer exercise test with VO 2 max measurement, fatigue assessment and objective and subjective disability parameter testing was performed on 155 patients (mean age 42.1 ± 9.9 years) classified into three groups: patients with chronic lower back pain, patients with an upper limb musculoskeletal disorder, and patients with multifocal chronic pain.
Results
The mean VO 2 max value was 22.18 mL/min/kg. There was no statistically significant difference in VO 2 max between the three groups. The patients with poorest aerobic condition were older ( P < 0.007), were on sick leave longer ( P < 0.03), had weaker Sorensen test ( P < 0.01) and P.I.L.E. ( P < 0.004) results, had more perceived fatigue ( P < 0.04), a higher mean BMI ( P < 0.0001) and gained more weight during sick leave ( P < 0.02).
Discussion
Numerous studies have examined loss of aerobic capacity due to chronic low back pain with contradictory results. This is probably due to variability of in the methods used to measure or calculate VO 2 max as well as to the variability in the studied populations.
Conclusion
It seems appropriate to offer patients with chronic pain multidisciplinary exercise rehabilitation programs.
Résumé
Objectif
Étudier la capacité aérobie de patients douloureux chroniques et rechercher des corrélations entre la VO 2 max et différents paramètres d’incapacité.
Population et méthodes
Épreuve d’effort sur cycloergomètre avec mesure de la VO 2 max, évaluation de la fatigue, évaluation des paramètres objectifs et subjectifs d’incapacité chez 155 patients (âge moyen 42,1 ± 9,9 ans) classés en trois groupes : lombalgique chronique, trouble musculosquelettique du membre supérieur et syndrome douloureux multifocal.
Résultats
La valeur moyenne de la VO 2 max était de 22,18 mL/min/kg, sans différence significative entre les trois groupes. Les patients les plus déconditionnés étaient plus âgés ( p < 0,007), avaient une durée d’incapacité plus longue ( p < 0,03), des résultats plus perturbés aux tests de Sorensen ( p < 0,01) et de P.I.L.E. ( p < 0,004), une perception de fatigue plus forte ( p < 0,04), un IMC plus élevé ( p < 0,0001) et une prise de poids plus importante ( p < 0,02).
Discussion
La discordance entre les nombreuses études portant sur la VO 2 max chez les lombalgiques chroniques peut s’expliquer par la variabilité méthodologique et l’hétérogénéité des populations étudiées.
Conclusion
Il nous semble licite de proposer aux patients douloureux chroniques des programmes multidisciplinaires de réadaptation à l’effort.
1
English version
1.1
Introduction
Deconditioning syndrome is described as one of the explanations for exercise intolerance and the progressive decline in physical capacity in chronic lower back pain patients , and especially in such patients when they are on prolonged sick leave .
The VO 2 max is the maximum capacity of an individual’s body to transport and use oxygen during an incremental exercise. It reflects an individual’s physical condition. In chronic lower back pain patients, it is assumed that a progressive decline in physical activity affects maximal aerobic capacity, creating a real vicious cycle in which inactivity leads to aerobic deconditioning, which is responsible for a further decline in physical activity. However, there is contradictory data on this subject .
Several studies demonstrated that in chronic lower back pain patients, aerobic capacity, which is estimated by the VO 2 max calculated or measured during a submaximal exercise test, was lower than in healthy subjects . However, no statistically significant correlation could be established between this decline in aerobic capacity and different parameters, such as pain intensity, disability duration, level of activity during work, during daily living and during recreational activities, or negative cognition . Hoch et al. found that in women with chronic lower back pain, the VO 2 max measured during a maximal exercise test was lower than in control subjects . Ivan Duque et al. reported that, in chronic lower back pain patients, VO 2 max was comparable to that of healthy subjects in weak physical condition according to the classification suggested by Shvartz et al. . Other authors uphold that the aerobic capacity of chronic lower back pain patients is comparable to that of healthy subjects .
Moreover, it is questioned whether or not there is a correlation between a drop in VO 2 max and a decrease in physical capacity and the ability to perform daily activities in lower back pain patients. Brox et al. found an absence of statistically significant differences in VO 2 max in chronic lower back pain patients compared with a control group as well as an association with lower performance in terms of spinal extensor muscle endurance, as determined by the Sorensen test.
Deconditioning syndrome could also account for the decrease in physical activity in patients with musculoskeletal pain other than lower back pain. So far, there have been no studies conducted on this subject. Our main objective was to study the aerobic capacity of patients presenting with chronic pain of varying etiologies (chronic lower back pain, upper limb musculoskeletal disorders and multifocal chronic pain), and to determine whether or not there was a difference according to etiological group or if the low aerobic capacity was a trait common to all chronic pain phenomena. The secondary objectives were to search for correlations between the level of aerobic capacity of these patients and different subjective and objective disability parameters.
1.2
Materials and methods
1.2.1
Population
All patients admitted to the unit for a chronic pain syndrome workup or for rehabilitation generally undergo an exercise test with VO 2 max measurement through indirect calorimetry. Patients over the age of 50 or who have at least two cardiovascular risk factors undergo a pre-admission stress test with a cardiologist to rule out contraindications for an aerobic rehabilitation program.
All of the patients assessed in the Physical Medicine and Rehabilitation unit of the Château-Renault hospital between January 1st, 2010 and December 31st, 2012 were included in this study. There were no changes to the assessment generally performed in the unit. All of the patients were informed that the data would be processed according to the recommendations of the CNIL, or the French Commission for Information Technology and Civil Liberties (the opinion of the French Ethics Committee was not necessary since the assessment protocol and data analyses were not different from what is generally performed in the unit).
Out of 161 patients initially assessed (mean age 42.1 ± 9.9 years; 81 men and 80 women) in the Physical Medicine and Rehabilitation unit of the Château-Renault hospital, 155 patients who had a complete assessment were included in the study.
The patients included in the analysis were 18 to 60 years of age, were professionally active, on sick leave or unemployed, and had musculoskeletal pain that had been worsening for more than three months. Given the preliminary admission criteria, none of the patients were excluded.
These patients were classified into three groups according to the etiology of their pain ( Table 1 ):
- •
“chronic lower back pain” (CL): back pain with or without radiation to the lower limbs, and without any objective neurological compromise;
- •
“upper limb musculoskeletal disorders” (ULM) specific or non-specific pain of an upper limb;
- •
“multifocal chronic pain” (MCP): pain at several anatomical sites (at least lumbar pain and unilateral or bilateral ULM).
| Total population | CL | ULM | MCP | p | |
|---|---|---|---|---|---|
| n | 155 | 71 | 46 | 38 | |
| Age (years) | 42.1 ± 9.9 | 42.3 ± 9.1 | 39.8 ± 10.8 | 43.9 ± 10.1 | NS |
| Gender (M/F) | 77/78 | 50/21 | 15/31 | 12/26 | 0.0001 |
| BMI (kg/m 2 ) | 26.6 ± 5.7 | 26.8 ± 5.4 | 27.6 ± 6.4 | 24.9 ± 4.9 | NS |
| Duration of disability (months) | 9.9 ± 9.1 | 9.1 ± 7.1 | 11 ± 10.4 | 10.3 ± 10.6 | NS |
| Duration of disability ≥ 12 months | 66 (42.58%) | 30 (42.25%) | 21 (45.6%̈) | 15 (39.5%) | NS |
1.2.2
Methods
All subjects underwent the initial assessment usually conducted in the unit.
This assessment is multidisciplinary and conducted by PRM physicians, physical therapists and occupational therapists. The assessment comprised:
- •
a detailed interview about the history of the pain;
- •
a full clinical examination;
- •
a cycloergometer exercise test with VO 2 measurement. This was a progressive test starting at 30 W and increasing in 30 W increments lasting three minutes each. It was performed using a Cardiocontrol Ergometer ® . The pedaling speed was maintained at 60 revolutions/min for the duration of the test. It was explained to the patients that the objective was to achieve maximal performance despite the pain. The VO 2 measurement was performed using a MedGraphics Cardiorespiratory Diagnostic Systems ® gas exchange analyzer and the highest VO 2 value recorded during the test was used as the VO 2 max. The calibration of the measurement device was performed at the beginning of each session (a session included four to six exercise tests per half-day). The cardiac activity was monitored continuously throughout the test and the blood pressure was measured before starting the exercise test, at each incremental level and after three minutes of rest at the end of the test. The test was stopped either in the event of patient exhaustion (submaximal test) or if the theoretical maximum heart rate (TMHR), defined by the formula 220-age, was reached (maximal test). The VO 2 max values were expressed relative to body mass in mL/kg/min. The values were compared with the Schvartz classification system, by age group and by gender, with the values broken down into seven categories of aerobic condition: “one, excellent”, “two, very good”, “three, good”, “four, average”, “five, fair”, “six, poor”, “seven, very poor”.
The perceived exertion according to the Borg scale was assessed before exertion, after exertion, and after three minutes of rest.
The objective assessment of disability was performed as follows:
- •
using a Sorensen test : patients positioned in ventral decubitus position with the trunk unsupported, the lower limbs secured and the arms crossed over the chest must hold their trunk in horizontal position for as long as possible. This test helps assess the endurance of the spinal extensors;
- •
using a progressive iso-inertial lifting evaluation (P.I.L.E.) test developed by Mayer et al. ): the patient must lift a load from the floor to waist height four times in a row within a 20-second time period, starting with a 4 kg load and then increasing in 2.5 kg increments until they reach a level of severe discomfort. When the maximum load is reached, the percentage the load represents of body weight and total mass moved are recorded. Before the test, after the test and after three minutes of rest, the following were assessed: heart rate, blood pressure and perceived fatigue according to the Borg scale.
The assessment of subjective perceived disability using self-questionnaires: EIFEL for chronic lower back pain , DASH for upper limb pain , both self-questionnaires if the clinical table associated lower back pain with pain of at least one upper limb.
The patients were then classified into three groups based on the VO 2 max values relative to weight:
- •
group I: VO 2 max lower than 17 mL/kg/min;
- •
group II: VO 2 max between 17 and 25 mL/kg/min;
- •
group III: VO 2 max over 25 mL/kg/min.
Since the constitution of a control group was not feasible, the results obtained for our population were compared with the Shvartz classifications , which grouped the subjects according to seven categories of aerobic condition based on age, gender and VO 2 max. Category 1 corresponded to “excellent” aerobic condition, category 2 to “very good” aerobic condition, category 3 to “good” aerobic condition, category 4 to “average” aerobic condition, category 5 to “fair” aerobic condition, category 6 to “poor” aerobic condition and category 7 to “very poor” aerobic condition.
1.2.3
Statistical analysis
The comparisons of quantitative parameters were performed using the Student test. The comparisons of mean values based on the different categories were performed using the ANOVA test. The correlations between quantitative parameters were studied using a Statview correlation test. A difference was considered to be statistically significant if P is less than 0.05.
1.3
Results
1.3.1
Mean VO 2 max values
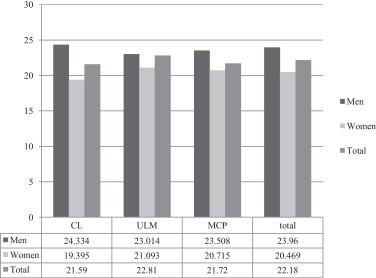
The mean VO 2 max value in relation to weight was 22.18 mL/min/kg (23.96 mL/min/kg in men and 20.46 mL/kg/min in women).
Ninety (90) patients (58.1%) had a submaximal exercise test (maximum heart rate during the test less than 95% of the TMHR) and 65 (41.9%) had a maximal exercise test (maximal heart rate during the test was greater than or equal to 95% TMHR). The early discontinuation of the exercise test was related neither to age nor to gender. In addition, it was not related to the perceived exertion before or at the end of the exercise test. Based on the VO 2 max value, the exercise test was maximal in six patients (23.1%) of group I, 34 patients (39.5%) of group II and 25 patients (58.1%) of group III patients ( P > 0.02).
The exercise test was accompanied by muscular intolerance (serum creatinine kinase levels of more than twice the normal level) in 8% of group I patients, 32.9% of group II patients and 35.9% of the group III patients ( P < 0.02, between the group I patients and the patients of the other two groups).
There was no statistically significant difference found for the VO 2 max value in relation to weight for the three etiological groups studied ( Fig. 1 ). In contrast, we observed a decrease in VO 2 max with age ( P > 0.004) and the mean VO 2 max value was significantly lower in women than in men ( P > 0.003).
When compared with the Shvartz classification, the mean VO 2 max corresponded to both male and female subjects in “very poor” physical condition. The study by age group and by gender demonstrated that the majority of patients (55.5%) were in the lowest category (7, or “very poor”); only 4.5% were in category 2 (“very good”) and category 3 (“good”), 10% in category 4 (“average”), 9% in category 5 (“weak”) and 20% in category 6 (“poor”). Neither age, nor gender, nor etiological group influenced these results.
With respect to the surgical history, since no patients had been admitted during the immediate post-operative period and there had been a recent period of prolonged bed rest, we decided that this item could not be a confusion factor. In the CL group, thirteen patients had undergone a herniated disc repair six months to 20 years previously, two patients had undergone a laminectomy – one 3 years previously and one 12 years previously, and one patient had undergone arthrodesis 10 years previously. Of the ULM, patients, three had been operated on for carpal tunnel syndrome three months to 3 years previously, one patient had undergone neurolysis and ulnar nerve transposition 6 years previously, two patients had undergone an acromioplasty 2 years previously and 12 years previously respectively, one patient had undergone a rotator cuff repair six months previously, one patient had undergone a distal clavicle resection 2 years previously and one patient had undergone epicondyle release 4 years prior to the rehabilitation. Finally, in the MCP group, seven patients had been operated on for carpal tunnel syndrome one to 6 years previously, four patients had undergone ulnar nerve release three months to 6 years previously, one patient had undergone an Achille’s tendon repair 2 years previously, one patient had undergone a laser nucleotomy 5 years previously, one patient had undergone ulnar nerve resection 4 years previously, one patient had undergone a herniated disc repair 3 years previously, one patient had undergone a rotator cuff repair 2 years previously and one patient had undergone a trigger finger repair 4 years prior to rehabilitation treatment.
1.3.2
Correlations between VO 2 max and the disability parameters
We compared the various disability and deconditioning indicators according to the VO 2 max value by separating the patients into the three groups described above ( Table 2 ). Compared with the patients of the two other groups, the patients of group I were older ( P > 0.007) and had a longer duration of professional disability ( P > 0.03).
| Group I n = 26 | Group II n = 86 | Group III n = 43 | P | |
|---|---|---|---|---|
| Mean age (years) | 45.8 ± 7.9 | 42.6 ± 10.1 | 38.4 ± 9.8 | 0.007 b |
| Men/Women | 8/18 | 39/46 | 29/14 | 0.01 |
| Duration of disability (months) | 13.9 ± 10.8 | 9.8 ± 9.2 | 7.9 ± 7.05 | 0.03 a |
| Maximum weight lifted during P.I.L.E. test (in kg) | 20.9 ± 9.5 | 25.5 ± 12.4 | 30 ± 11.9 | 0.02 b |
| Maximum weight lifted during P.I.L.E. test (% body weight) | 29.1 ± 15.7 | 32.6 ± 14.1 | 41.6 ± 15.5 | 0.004 a,c |
| Sorensen (seconds) | 134 ± 56 | 133 ± 60 | 158 ± 60 | 0.03 b |
| EIFEL | 10.4 ± 4.1 | 10.5 ± 5.1 | 9.2 ± 4.9 | NS |
| DASH | 87.2 ± 16.5 | 81.9 ± 19.9 | 80.5± 20.1 | NS |
a Statistically significant difference between the results of the group I patients and the results of the patients of the other groups.
b Statistically significant difference between the results of the group I and II patients and the group III patients.
c Statistically significant difference between the results of the patients of groups II and III.
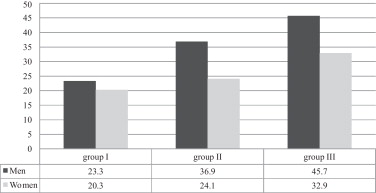
Furthermore, the results of the objective disability assessment tests were, in a statistically significant way, lower in patients with lower VO 2 max values: for the P.I.L.E. test, the mean maximum mass recorded, in percentage body weight, was lower for group I patients than for the patients of the two other groups ( P < 0.004), and the values obtained for the Sorensen test were lower for the group I and group II patients than for the group III patients ( P < 0.01). The analysis based on gender demonstrated that the mean values of the mass recorded in percentage body weight for the P.I.L.E. test were significantly different for men and women (38.8 ± 17.1% and 24.8 ± 11.8% respectively, P < 0.0001), and that the mean values for each of the groups were independent of gender ( Fig. 2 ).
In contrast, the subjective disability indicators did not demonstrate any statistically significant differences in perceived disability among the patients of the three groups.
With respect to perceived exertion measured according to the Borg scale, the group I patients more frequently perceived heavy exertion than the patients of the other two groups: 91% of the group I patients had a Borg scale score of 5 or higher (exertion perceived as ranging from “hard” to “extremely hard”) at the end of the exercise test, versus 73% of the group II patients and 61% of the group III patients ( P < 0.04) ( Table 3 ). There was no significant correlation between the Borg scores of the exercise test and the Borg scores for the P.I.L.E. and Sorensen tests, and likewise between the DASH and EIFEL scores.
| Group I n = 26 | Group II n = 85 | Group III n = 43 | |
|---|---|---|---|
| Borg < 5 (%) | 9.1 | 27 | 39 |
| Borg 5 to 7 (%) | 59.1 | 34.3 | 30.5 |
| Borg > 7(%) | 31.8 | 38.7 | 30.5 |
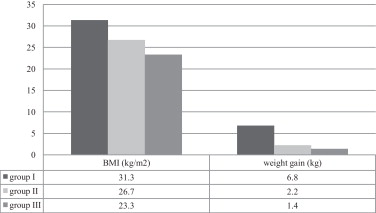
Finally, the group I patients had a mean Body Mass Index (BMI) of 31.3 kg/m 2 , corresponding to type I obesity, which was significantly higher than the patients of the two other groups ( P < 0.0001). Moreover, they had a mean weight gain of 6.8 kg during the sick leave preceding hospitalization, which was significantly higher than for the group II and group III patients ( P < 0.02) ( Fig. 3 ).
1.4
Discussion
Our study is the first that looks at VO 2 max measurements in patients with pain other than chronic lower back pain. In chronic pain patients, regardless of their etiology, we found a low mean VO 2 max, although a statistically significant difference between the three etiological groups could not be demonstrated. The study by age range and by gender showed that 75.5% of our patients were classified in Shvartz category 6 (poor physical condition) or 7 (very poor physical condition). Only 4.5% of the population was classified above the mean physical condition. These results evidenced aerobic deconditioning in the entire study population, regardless of the etiology of the chronic pain syndrome; no other study has ever demonstrated this.
However, we cite Nielens et al. , who assessed the cardiorespiratory fitness by the physical work capacity at 65% of the theoretical maximum heart rate in relation to weight (PWC65%/kg) during a cycloergometer exercise test, as well as the level of physical activity (by the Baecke questionnaire) in patients with chronic pain of various etiologies (chronic lower back pain, fibromyalgia, cervicalgia, dorsalgia, neuropathic pain, cephalalgia) versus healthy subjects. They found a statistically lower PWC65%/kg in chronic pain subjects than in healthy subjects, and no correlation between level of physical activity and aerobic capacity could be revealed.
However, many studies were on the measurement or calculation of VO 2 max in chronic lower back pain patients ( Table 4 ) with conflicting results. We compared the results of these studies to the Shvartz classification : the VO 2 max levels found by the various authors corresponded to a physical condition ranging from “good” to “very poor”, with the exception of Smeets et al. , who found a VO 2 max of 44.8 mL/kg/min in female chronic lower back pain patients, which corresponded to an “excellent” physical condition for the age category. Furthermore, some of these studies compared the VO 2 max of chronic lower back pain patients to those of a control group. There was a predominant statistically significant difference that was negative for the test group . However, Brox et al. did not find a statistically significant difference between the chronic lower back pain patients and a control group matched for gender and age. Rasmussen-Barr et al. did not find a statistically significant difference between the VO 2 max of 57 female lower back pain patients who had not interrupted their professional activity and 57 healthy female subjects matched for gender and age.
| Author | Study population | Control population | Method of measurement | VO2max (mL/kg/min) M/F | Comparison with the Shvartz classification (Shvartz and Reibold, 1990) a | Comparison with the control population |
|---|---|---|---|---|---|---|
| Brennan et al. (1987) | 40 herniated disc patients recruited in a neurosurgery clinic | 40 healthy subjects matched for gender and age | Submaximal cycloergometer exercise test, calculation of VO2max according to Astrand method | 30.2/25.3 mL/kg/min Mean: 28.9 mL/kg/min | Fair physical condition (6) | Statistically poorer than the control population (for both genders) |
| Mc Quade et al. (1987) | 96 chronic lower back pain patients (> 6 months), referred by physical therapists or chiropractors, or who came after seeing a media advertisement | Submaximal cycloergometer exercise test, calculation of VO2max according to the Astrand method | Mean = 20.5 mL/kg/min | Very poor physical condition (4) | ||
| Davis et al. (1992) | 46 patients starting a rehabilitation program for chronic pain | Cycloergometer exercise test, VO2max measurement by indirect calorimetry | Mean = 16.2 mL/kg/min | Very poor physical condition (7) | ||
| Robert et al. (1995) | 30 patients (27 men and 3 women) starting a rehabilitation program for chronic lower back pain | Submaximal cycloergometer exercise test, VO2max calculation | Mean = 30.49 mL/kg/min | Poor physical condition (6) b | ||
| Wittink et al. (2000) | 50 chronic lower back pain patients | Treadmill exercise test, VO2 peak measurement by indirect calorimetry, VO2max calculation by extrapolation if not achieved during the test (92%) | 39.3/30.9 | Average physical conditioning (4) | ||
| Van der Velde et al. (2000) | 137 chronic lower back pain patients | Submaximal step test, calculation of VO2max according to the CSTF (Canadian Standardized Test of Fitness) | Lower VO2max level than the 1981 CFS norms (on average, 19.64 th percentile) | |||
| Wittink et al. (2002) | 75 chronic lower back pain patients (> 3 months) referred for rehabilitation treatment | Treadmill exercise test, VO2 peak measurement by indirect calorimetry, VO2max calculation by extrapolation only if not achieved during the test. | 38.7/33.46 | Average physical conditioning (4) | ||
| Brox et al. (2005) | 46 sub-acute lower back pain patients (8 to 12 weeks), 45 chronic lower back pain patients | 45 control subjects matched for gender and age | Submaximal cycloergometer exercise test, calculation of VO2max according to the Astrand method | Chronic lower back pain: 31.8 sub-acute lower back pain: 30.7 | No statistically significant difference in VO2max between the three groups | |
| Hoch et al. (2006) | 21 chronic lower back pain patients (> 1 year) | 20 female control subjects | Treadmill exercise test, VO2max measurement by indirect calorimetry | 35.8 | Good physical condition (3) | Statistically significant difference between the two groups |
| Smeets et al. (2006) | 108 chronic lower back pain patients (> 3 months) | Normative population matched for age, gender and physical activity level (database | Submaximal cycloergometer exercise test, calculation of VO2max according to the Astrand method | 40/44.8 | Fair physical condition (5) for the men, excellent for the women (1) | Statistically significant difference between the two groups |
| Rasmussen-Barr et al. (2008) | 57 lower back pain patients who did not interrupt their professional activity | 57 control subjects matched for gender and age | Maximal cycloergometer exercise test, calculation of VO 2 max according to Astrand method | 38.1/33.6 | Average physical conditioning (4) | Statistically significant difference between the two groups in women only |
| Duque et al. (2009) | 100 chronic lower back pain patients | Cycloergometer exercise test, VO 2 max or VO 2 peak measurement by indirect calorimetry | 31.9/27.1 (if the VO 2 max criteria are present: 34.1/28.4) | Fair physical condition (5) | ||
| Duque et al. (2011) | 70 chronic lower back pain patients (> 6 months, sick leave > 4 weeks) | 101 asymptomatic subjects | Maximal cycloergometer exercise test, VO 2 max measurement by indirect calorimetry | 33.9/22.7 | Fair physical condition (5) for the men, poor for the women (1) | VO 2 max significantly lower than in the control population |
Related posts:
 Activité physique et MPR
Non-pharmacological strategies in cardiovascular prevention: 2011 highlights
Therapeutic education in cardiovascular diseases: State of the art and perspectives
Accelerometer as a tool to assess sedentarity and adherence to physical activity recommendations after cardiac rehabilitation program
Le Congrès MPR Sofmer 2010 Marseille à l’heure des bilans
Filiarisation de l’internat et refonte du troisième cycle : un nouveau souffle pour la médecine physique et de réadaptation en France
Activité physique et MPR
Non-pharmacological strategies in cardiovascular prevention: 2011 highlights
Therapeutic education in cardiovascular diseases: State of the art and perspectives
Accelerometer as a tool to assess sedentarity and adherence to physical activity recommendations after cardiac rehabilitation program
Le Congrès MPR Sofmer 2010 Marseille à l’heure des bilans
Filiarisation de l’internat et refonte du troisième cycle : un nouveau souffle pour la médecine physique et de réadaptation en France
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


