Fig. 1.1
Preoperative virtual planning. Pelvis tumor planned with 3 planes
Advantages
Obtain real anatomic three-dimensional information.
Compare conventional 2D images with 3D models.
Interact with 3D models.
Plan an oncological margin in a three-dimensional environment.
Plan an osteotomy, surgical approach or place an implant.
Drawbacks
This study cannot be done optimally with images acquired for diagnosis. 3D reconstructive resolution is subjected to the way in which the image has been acquired in tomography and MRI. To reach an adequate resolution in 3D we need to adjust acquisition for tomography images and MRI protocol within 1 mm or smaller cuts and modify some other specific parameters of reconstructing three-dimensional relevant regions.
Moreover, some VPP limitations are due to the tomography or MRI, such as oncology margin determination. This is going to be limited on what we call suspicious image in nuclear magnetic resonance (MRI). Tumour images in MRI is an indirect acquisition, that is, we can only see a shadow left by the tumour in healthy tissue and we cannot see tumour activity site in the image directly. Although positron emission tomography (PET Scan) allows to see cellular activity, the image is not accurate enough for millimetre oncology margin measurement. Suspicious images can also be generated due to MRI signal changes by peri-tumoral liquid, post chemotherapy changes or radiotherapy. In this case, specialists are to define definitive oncology margin limits in MRI.
Instructions
First VPP instruction is on tumour injuries either to state the length in big injuries or anatomic three-dimensional situation in smaller injuries [6].
Visualizing tumour location before surgery in anatomic space is useful to take decisions about surgical techniques.
Head and neck cases in need of VPP are usually tumours located in complex anatomic sites, generally demands several medical specialists teams.
Holding meetings involving different specialists turns VPP into a tool for exchanging knowledge between several fields and help diagramming surgical logistic (Fig. 1.2).
Fig. 1.2
(a) Preoperative planning meeting defining margins and planar conformation. (b) Surgeon in OR, executing the osteotomy previously planned
At these meetings issues about patient positioning, boarding and types of instruments are discussed. This kind of information helps to diagram and organize surgical methodology at complex interventions. In other words, we are indirectly saving time in the operating room and leading to a more predictable procedure (Fig. 1.3). This techniques affect directly on the quality of the intervention.
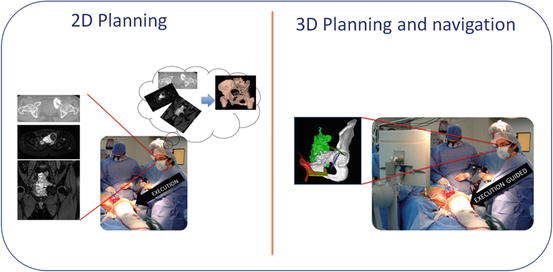
Fig. 1.3
Two dimensional planning implies an extra mental effort. However virtual navigation allows to surgeons to apply 3D Planning previously planned
What Is Virtual Preoperative Planning?
In order to obtain a VPP it is necessary to recreate anatomic structures in 3D.
Related posts:

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


