Varus and Valgus (Crossover) Lesser Toe Reconstruction
Scott Riester
Ari Kaz
Michael Coughlin
Crossover toe deformity is a lesser toe deformity that is a distinct entity from hammer toe and claw toe (1, 2, 3 and 4). It occurs when a lesser toe, typically the second, deviates medially and dorsally over the dorsum of the great toe (Fig. 10.1). In comparison to the uniplanar instability associated with hammer toe and claw toe deformities, crossover toe results in multiplanar instability at the second metatarsophalangeal (MTP) joint. The deformity often begins with mild pain and synovitis involving the second MTP joint. As the deformity progresses, the ligamentous and capsular structures become either stretched or contracted; this eventually progresses to attenuation of the plantar plate resulting in global instability at the second MTP joint (2,5, 6, 7, 8, 9 and 10).
Dorsomedial subluxation of the second toe has a high association with other deformities, including hallux valgus, hallux rigidus, and hammer toe deformities. Intrinsic factors such as muscle imbalance and second metatarsal length are thought to contribute to the development of deformity. Acute and repetitive trauma, inflammatory arthritides, constrictive footwear, and adjacent toe deformities represent extrinsic factors that are believed to contribute to the development of crossover toe deformity.
Crossover toe deformity has historically been a challenging problem to treat. Countless surgical techniques have been described, with no clear consensus as to which technique is most effective (11, 12, 13, 14, 15, 16 and 17). The large number of surgical techniques that have been developed to treat this problem simply highlights the challenges that face the treating surgeon. Surgical management of crossover toe deformity has evolved over the years from soft tissue procedures alone, to the addition of tendon transfers, to soft tissue releases combined with osteotomies, and to the combined use of tendon transfers with osteotomies. Resection arthroplasty of the base of the phalanx or of the metatarsal head, proximal phalangeal closing wedge osteotomy, and second toe amputation have also been performed. In this chapter, two surgical techniques are discussed: extensor digitorum longus (EDL) to extensor digitorum brevis (EDB) tendon transfer, and a shortening osteotomy with EDB tendon transfer.
INDICATIONS AND CONTRAINDICATIONS
It is important to distinguish between a crossover toe deformity and a hammer toe or claw toe deformity. A crossover toe has multiplanar instability whereas a claw toe or hammer toe has only stability in one plane. If a crossover toe is not recognized and improperly treated as a hammer toe or claw toe, then treatment failure is likely.
The most common presenting complaint in a patient with crossover toe deformity is a painful corn dorsally over the proximal interphalangeal (PIP) joint or vague pain at the second MTP joint. In the
early stages of this disorder, there may only be minimal medial deviation of the second toe. The patient may report a feeling of thickness or swelling in the area of the second MTP joint, and may report the sensation of walking on a pebble or bunched-up sock. A neuroma in the second webspace should be considered in the differential diagnosis. Injections of local anesthetic can be helpful in differentiating between a neuroma and second MTP synovitis.
early stages of this disorder, there may only be minimal medial deviation of the second toe. The patient may report a feeling of thickness or swelling in the area of the second MTP joint, and may report the sensation of walking on a pebble or bunched-up sock. A neuroma in the second webspace should be considered in the differential diagnosis. Injections of local anesthetic can be helpful in differentiating between a neuroma and second MTP synovitis.
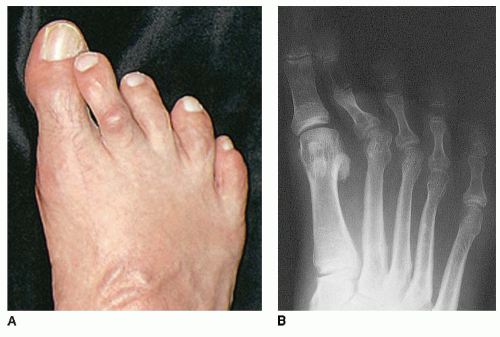 FIGURE 10.1 A: Clinical photograph of a crossover toe deformity. B: Anteroposterior (AP) foot radiograph. |
To aid in diagnosis the drawer test can be used to test for stability of the affected MTP joint. This is performed by dorsiflexing the involved toe to 25° and applying a dorsal force to the toe. Laxity and pain with this maneuver is caused by attenuation of the plantar plate and collateral ligaments. Additionally, a callus may be present on the plantar surface of the affected toe or over the dorsum due to impingement on the toebox of footwear.
Standing anterior posterior, oblique and lateral radiographs of both feet should be obtained. These may reveal subtle joint space widening due to synovitis in the early stages of the disease, and later may show obvious medial deviation at the second MTP joint (see Fig. 10.1B).
Nonoperative measures should be considered first; these include the use of anti-inflammatory medications, corticosteroid injection into the second MTP joint, and footwear modification to accommodate the deformity. The shoe upper should be made of softer, flexible material, and stretched over the prominence with a ring and ball stretcher. A pad or silicone sleeve may be used over the second toe to reduce pain and corn formation. The affected toe may be taped to the adjacent toe in a more aligned position. Orthotics with excavation under the metatarsal head may be used when the predominant symptom is metatarsalgia. When conservative management fails to provide adequate pain relief, surgical treatment can be considered.
Relative contraindications to surgery include peripheral vascular disease, diabetes mellitus, and an immunocompromised patient. Other contraindications include infection, inability to maintain protected weight bearing, and severe vascular insufficiency of the toes.
PREOPERATIVE PLANNING
The weight-bearing radiographs should be carefully studied prior to surgical intervention. If symptomatic hallux disorders are present, these could be corrected to provide adequate room for correction of the second toe. The length of the second metatarsal should be evaluated in relation to the neighboring metatarsals. The second metatarsal should be at approximately the same level as the first metatarsal, and should follow the normal decreasing metatarsal length cascade. If the second metatarsal is too long, then a shortening osteotomy should be considered. The amount of shortening required to bring the second metatarsal into alignment with the rest of the metatarsal should be determined by measurements taken from the preoperative radiographs.
SURGICAL TECHNIQUES
Technique 1: Extensor Digitorum Longus to Extensor Digitorum Brevis Transfer For Varus/Valgus Lesser Toe Deformity
The patient is supine, and ankle block anesthesia is administered. An Esmarch bandage is used as a tourniquet.
An incision is made dorsally starting over the PIP joint of the second toe and extended 5 cm proximally in line with the metatarsal shaft to expose the EDL and EDB tendons (Fig. 10.2).
An EDL Z-lengthening is performed. It is important to ensure that long limbs are created so that there is adequate length to reroute the tendon (Fig. 10.3).
The EDL is detached from the dorsal capsule and the extensor hood from its insertion to 4 cm proximal to the MTP joint.
The EDB is sectioned at the distal metatarsal level distal to the musculotendinous junction.
The dorsal capsule, medial collateral ligament, and associated lumbrical are completely released. The medial capsular release should extend deep but should not involve sectioning of the medial plantar plate (Fig. 10.4).
If necessary, the plantar plate at the site of its origin on the distal metatarsal should be incrementally released until axial alignment of the toe is achieved.Related posts:
 Hallux Metatarsophalangeal Interposition Arthroplasty (Modified Keller Procedure)
Hallux Metatarsophalangeal Interposition Arthroplasty (Modified Keller Procedure)
 Plantar Interdigital Neuroma Resection: Primary and Revision
Plantar Interdigital Neuroma Resection: Primary and Revision
 Medial Displacement Osteotomy of the Calcaneus and Flexor Digitorum Longus Transfer
Medial Displacement Osteotomy of the Calcaneus and Flexor Digitorum Longus Transfer
 Peroneal Tendon Repair and Reconstruction
Peroneal Tendon Repair and Reconstruction
 Tibiofibular Syndesmosis Reduction and Fixation
Tibiofibular Syndesmosis Reduction and Fixation
 Autologous Osteochondral Transfer for Talar Defects: Mosaicplasty
Autologous Osteochondral Transfer for Talar Defects: Mosaicplasty

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


