Use of the Extended Trochanteric Osteotomy in Revision Total Hip Arthroplasty
Brett R. Levine
Darwin Chen
Case Study
A 47-year-old male presents with severe left thigh pain 1 year after total hip arthroplasty (THA) performed for a subtrochanteric femur fracture after a gunshot wound and a cephalomedullary nail was utilized for fixation (Fig. 104.1). An extended trochanteric osteotomy (ETO) was planned to assist with bypassing the distal pedestal, facilitate preparation of the femoral canal for the revision stem, and avoid difficulties secondary to the greater trochanter overhanging the shoulder of the femoral component, prohibiting simple extraction.
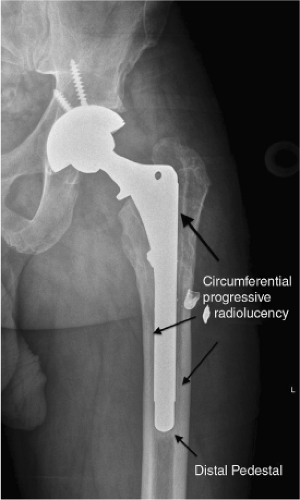 Figure 104.1. AP left hip with loosening (as evidenced by the circumferential progressive radiolucency–3 arrows), distal pedestal formation (lower arrow). |
Introduction
The number of patients requiring revision total hip arthroplasty (THA) continues to increase due to the tremendous number of indwelling implants and the greater number of primary surgeries performed yearly. Femoral revision surgery can be a complex and challenging task depending on the etiology of failure and remodeling of the proximal femoral anatomy. Similarly, complex primary THA scenarios exist in which the proximal femoral anatomy is severely distorted, hardware requires removal or prior osteotomy was performed. In such cases the use of an ETO may greatly facilitate the surgical procedure and prevent complications associated with these complex procedures including compromised host bone, osteolysis, severe remodeling, and weakened host bone after removal of hardware or well-fixed cementless and cemented stems (1,2,3,4).
When greater surgical exposure is necessary an ETO is an extremely useful tool in the armamentarium of hip surgeons. Originally described in 1991, by Cameron, for a case with greater trochanteric overhang in association with a loose femoral stem and a poor bed of reattachment for a standard trochanteric osteotomy (5). The technique involves a posterior or anterolateral exposure with an osteotomy that originates from the tip of the greater trochanter and extends distally to the extent needed to safely remove the femoral component, cement, pedestal or correct proximal femoral remodeling yet still retain sufficient bone stock for femoral component fixation. The osteotomy fragment encompasses approximately one-third of the proximal femoral diameter, maintaining the integrity of the vastus lateralis and abductor musculature
(Fig. 104.2). Compared to other osteotomies of the greater trochanter (Chevron/Charnley trochanteric osteotomy, anterior trochanteric osteotomy, trochanteric flip, and trochanteric slide), the ETO affords the most extensile exposure while minimizing the risk of trochanteric escape by keeping the muscle-osseous sleeve of the abductor-vastus lateralis and lateral femoral cortex intact (6). This technique is relatively straightforward to perform, can be readily repaired, and reliably heals with a low complication rate.
(Fig. 104.2). Compared to other osteotomies of the greater trochanter (Chevron/Charnley trochanteric osteotomy, anterior trochanteric osteotomy, trochanteric flip, and trochanteric slide), the ETO affords the most extensile exposure while minimizing the risk of trochanteric escape by keeping the muscle-osseous sleeve of the abductor-vastus lateralis and lateral femoral cortex intact (6). This technique is relatively straightforward to perform, can be readily repaired, and reliably heals with a low complication rate.
The modern form of the osteotomy was later popularized by Paprosky et al. (3). Advantages of the ETO include maintenance of proximal femoral bone stock, predictable healing, allows for tensioning of the abductors, and provides extensile exposure of the hip. Potential concerns include trochanteric escape, osteotomy nonunion/malunion, recalcitrant bursitis, and fragmentation of the osteotomy (1,7).
Indications
The indications for an ETO include the following (Fig. 104.3):
Removal of a well-fixed, fully porous-coated or extensively coated cementless stem
Removal of a well-fixed cemented stem
Distal cement mantle, plug or pedestal removal
Femoral revision with proximal femoral deformity (i.e., varus remodeling; Fig. 104.4)
Need for extensile acetabular exposure
All of the above in the face of periprosthetic fracture or infection
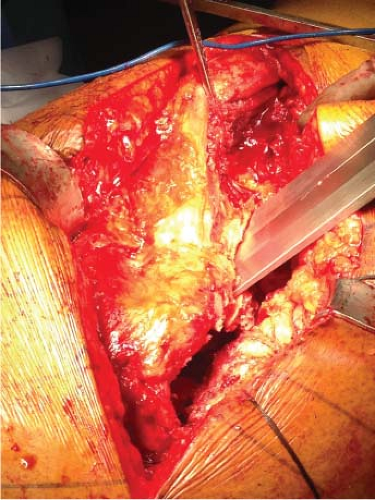 Figure 104.2. Intraoperative image at the time of ETO showing the abductor musculature and vastus lateralis are intact. (Image courtesy of Craig J. Della Valle, MD.) |
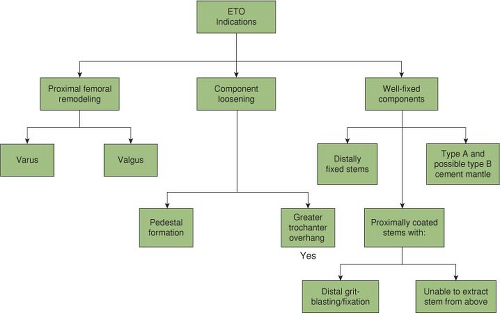 Figure 104.3. ETO indications. |
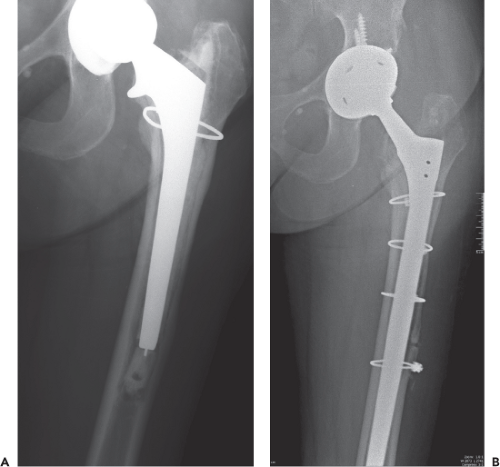 Figure 104.4. A: Loose femoral stem with varus remodeling of the femur. B: ETO utilized to place long stem component and correct the proximal femoral remodeling into varus. |
Relative contraindications for an ETO include femoral revision using impaction grafting technique, poor proximal femoral bone quality, and cemented femoral revision.
Operative Technique
Preoperative Planning
Establishing a thorough preoperative plan is crucial to the clinical outcome and must be based on sound principles (8). Preoperatively, complete radiographs of the pelvis, hip, and femur should be obtained. The surgeon should plan the distal extent of the osteotomy based on the following factors; the osteotomy should be long enough to facilitate component or cement mantle extraction while preserving 4 to 6 cm of femoral diaphysis distal to the ETO site to allow for adequate fixation (scratch fit) of the revision stem (Fig. 104.5). Additional consideration is necessary when dealing with a pedestal as this sclerotic intramedullary bone can ultimately result in eccentric reaming and possibly cortical perforation. In our case example, an ETO was performed to prevent greater trochanteric fracture with stem removal as well as to give us direct access to the bony pedestal.
Identification of the femoral component to be removed is important, to understand at what level the porous coating stops to determine how distal the osteotomy needs to be to easily remove the implant (Fig. 104.6). Similarly for removal of cemented femoral components, while a polished
stem may be easily removed from the cement mantle, a precoated or roughened cemented stem will require an ETO for safe removal. Femoral stem templates are then utilized in the planning process to determine if proximal femoral remodeling is present. When potted distally if the template reveals a “conflict” proximally with the anatomy, then either valgus or varus remodeling has occurred which can be corrected with an ETO (Fig. 104.4). With a fluted, tapered revision stem design (i.e., Wagner), the necessary amount of diaphyseal fit is less important but still must be considered. In general, the length of the osteotomy is at least 10 cm long and more typically is 12 to 15 cm long, measured from the tip of the greater trochanter.
stem may be easily removed from the cement mantle, a precoated or roughened cemented stem will require an ETO for safe removal. Femoral stem templates are then utilized in the planning process to determine if proximal femoral remodeling is present. When potted distally if the template reveals a “conflict” proximally with the anatomy, then either valgus or varus remodeling has occurred which can be corrected with an ETO (Fig. 104.4). With a fluted, tapered revision stem design (i.e., Wagner), the necessary amount of diaphyseal fit is less important but still must be considered. In general, the length of the osteotomy is at least 10 cm long and more typically is 12 to 15 cm long, measured from the tip of the greater trochanter.
 Figure 104.5. Planned ETO to afford adequate exposure for extraction (to a level near the end of the grit-blasted portion of the stem), yet still afford maximal distance for scratch fit upon reimplantation. |
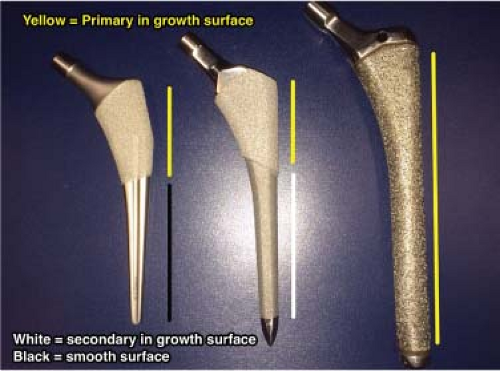 Figure 104.6. Proximally coated stem with smooth distal segment (left). Proximally coated stem with grit blasting below porous coating (middle). Fully coated stem (right). |
In the event that a cemented femoral component will be utilized for the reconstruction it is important to plan preoperatively to fix the osteotomy site prior to the cementation process. In addition, various adjuncts can be used to fill the gaps in the osteotomy to prevent cement extravasation as well as afford adequate canal pressurization. Similarly, impaction grafting can be performed in conjunction with an ETO, however, limited data is available as to the overall success of combining these techniques (9). The use of cement in conjunction with an ETO should be used cautiously as a recent retrospective review found that trochanteric osteotomies were three times more likely to develop a nonunion when cemented stems were used (10).
Surgical Technique
An ETO can be executed at various stages of the operation (1). It may be performed prior to hip dislocation if the hip cannot be dislocated from the acetabulum, however this is technically quite difficult (2). More commonly, the ETO is performed after the hip is dislocated but prior to removal of a well-fixed femoral component (3). Perhaps the easiest scenario is to perform an ETO after the hip is dislocated and after the femoral component has been extracted. However, one must be careful without a stem in place not to perforate through the anterior cortex with the saw as this may result in vascular injury.
ETOs are most commonly performed via a posterior exposure; however, it is possible from an anterior, anterolateral, or direct lateral approach (11,12,13). Adequate exposure of the femur is a requisite before initiating an osteotomy, and must include sufficient distance distally to complete the bony cuts. Utilizing a standard posterior approach the short external rotators, capsule, and scar are elevated and retracted posteriorly to protect the sciatic nerve. From a posterior approach, the hip is placed in extension and internal rotation. The lateral shoulder of the femoral prosthesis is cleared of all scar tissue and the inner aspect of the greater trochanter should be visible. After measuring from the tip of the greater trochanter the length of the proposed ETO, the vastus lateralis and vastus intermedius are gently elevated off of the linea aspera and reflected anteriorly to expose the distal extent of the preplanned osteotomy. To promote healing of the osteotomy care must be taken to not strip the entirety of the muscles from their attachment to the lateral femur. Excessive soft tissue stripping will compromise the vascular status of the bony segment and can lead to trochanteric nonunion and escape.
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


