Abstract
Objective
To document the effect of Postural Reconstruction ® physiotherapy on two postural disorders commonly observed in adolescents: genu varum and idiopathic scoliosis.
Patient and methods
A case report on a 16-year-old boy suffering from knee pain and presenting with bilateral genu varum and mild scoliosis. At the initial evaluation (T0), the intercondylar space was 7 cm and the Cobb angles for the right lumbar curve and left thoracic curve were 18° and 13°, respectively. The boy was treated with Postural Reconstruction ® , a neuromuscular physiotherapy intervention using facilitation/inhibition techniques. The outcomes used to quantify the effect of 6 months (T1), 12 months (T2) and 26 months (T3) of treatment were pain levels, the intercondylar space, the lumbar gibbosity and the lumbar and thoracic Cobb angles.
Results
The knee pain disappeared rapidly. At T3, the intercondylar space had decreased by 4 cm, the lumbar gibbosity angle had decreased by 2° and the lumbar and thoracic Cobb angles had decreased by 8° and 7°, respectively.
Conclusion
This non-invasive physiotherapy intervention appears to have considerable promise for the long-term correction of postural disorders.
Résumé
Objectif
Documenter les effets d’une intervention physiothérapique sur deux troubles posturaux fréquemment observés chez les adolescents : genu varum et scoliose idiopathique.
Patient et méthode
Ce rapport présente le cas d’un adolescent de 16 ans qui présente lors de l’évaluation initiale des gonalgies, un genu varum bilatéral asymétrique avec un écart intercondylien de 7 cm, une scoliose idiopathique lombaire droite de 18° d’angle de Cobb et thoracique gauche de 13°. Le patient est traité par la méthode physiothérapique de Reconstruction Posturale ® . Cette méthode, sélectionnée en raison du caractère multifocal du trouble postural, repose sur un processus de facilitation neuromusculaire. Les critères de jugement ayant servi à quantifier les effets de l’intervention à six mois (T1), 12 mois (T2) et 26 mois (T3) après le début de l’intervention sont : la mesure de l’intensité des algies, de l’écart intercondylien, de la gibbosité lombaire et des angles de Cobb.
Résultats
La résolution des gonalgies a été rapide et complète. À T3, l’écart intercondylien est réduit de 4 cm, la gibbosité lombaire de 2°, les angles de Cobb lombaire et thoracique, respectivement de 7° et de 8°.
Conclusion
Cette intervention non invasive semble prometteuse pour la réduction pérenne de ces troubles posturaux.
1
English version
1.1
Introduction
Genu varum and idiopathic scoliosis are commonly observed postural disorders in adolescents. In boys, genu varum may be more frequent than genu valgum . A genu varum morphotype is considered to require treatment when the intercondylar distance is greater than 5 cm or when the femur-tibia angle is negative . In the adolescent, surgery is only indicated when the deformity is severe or persists beyond the age of 11 or 12 . This deformity constitutes a biomechanical risk factor for knee osteoarthritis and aggravates the latter by increasing the load on the medial compartment . In France and the United States, knee osteoarthritis constitutes a public health problem . Although muscle strength training (for the abductors, hip adductors and quadriceps) relieves pain and improves function, it does not correct the varum misalignment .
Adolescent idiopathic scoliosis is defined as the presence of spinal curvature with a Cobb angle greater than 10°. The prevalence of this condition has been estimated at between 1% and 3% in the 10–16 age class . During adolescence, lumbar scoliosis may progress less rapidly than thoracic or thoracolumbar scoliosis. Right lumbar apex curves may nevertheless progress twice as quickly as left apex lumbar curves . In adulthood, lumbar scoliosis is likely to progress into rotatory dislocation and lumbar kyphosis – both of which are known to cause hard-to-treat pain . An international consensus is emerging with regard to the indications for surgery in scoliosis in the growing adolescent whose Cobb angle is greater than 45–50° . The value of conservative treatments (and notably physiotherapy) is subject to debate. Researchers in Europe suggest that self-administered physical exercises in all three planes of movement have a positive influence on scoliotic curvature , whereas North American experts consider that physiotherapy’s ability to modify the course of scoliosis has not been proven .
This article reports the effects of physiotherapy on a 16-year-old boy with these two postural disorders:
- •
bilateral genu varum with left predominance and knee pain;
- •
idiopathic right lumbar curve with non-structural, left thoracic curve.
In view of the presence of multifocal postural disorders, we decided to use Postural Reconstruction ® physiotherapy. This intervention used a therapeutic tool called “normalizing induction” and is based on neuromuscular facilitation/inhibition mechanisms . “Normalizing induction” has the advantage of avoiding the direct manipulation of painful areas. Postural Reconstruction ® can be applied on an out-patient basis, with no more than one session a week. Furthermore, the absence of self-administered exercises avoids the previously reported risk of poor treatment compliance with home-based therapies .
1.2
Patient and method
1.2.1
The case report
A 16-year-old male had been suffering from predominantly right side peripatellar pain for the previous 3 months. At rest, pain was absent. However, pain was felt when climbing stairs and prevented the patient from doing taekwondo. The mean pain intensity on a visual analogue scale (VAS) was 40 mm on the right side and 20 mm on the left. The patient felt recurrent, pain-free cracking when flexing his right knee. The orthopaedist diagnosed laxity of the knee, which translated into bilateral (but predominantly left-side) genu recurvatum during stance and bilateral (but predominantly left-side) tibia vara. Squinting patella was observed when the patient stood in closed stance. Lateral tibial torsion (measured according to Engel and Staheli’s method) was accentuated , with 60° on the left and 45° on the right (compared with normative values of between 25° and 40°) . Femoral torsion was normal on both sides. Femoral-patellar X-rays did not show any signs of osteochondritis. Radiographic measurements of the legs confirmed the asymmetric varum (6° on the left and 4° on the right). The intercondylar distance (measured from the front, with the patient standing in closed stance) was 7 cm. Given the absence of severe functional impairment, surgery was ruled out.
Idiopathic scoliosis was diagnosed during the patient’s first visit to the orthopaedist: a right lumbar curve with spinal rotation (T12-L4) and a Cobb angle of 18° and a left thoracic curve in the absence of spinal rotation (T7-T11) and with a Cobb angle of 13°. A right paraspinal lumbar gibbosity was present. The angle of trunk rotation was 7° (the patient was using a low heel to compensate for a 7 mm rightward pelvic imbalance). The neurological examination was normal. There was no spinal pain. The patient was Risser grade 2 and measured 170.5 cm in height. The criteria for use of a spinal orthosis were not met. Since the boy was still growing, 6-monthly radiological monitoring was recommended. The orthopaedist also recommended treatment of the postural disorders with Postural Reconstruction ® physiotherapy.
1.2.2
The Postural Reconstruction ® physiotherapy intervention
A series of treatment goals were agreed with the patient and his parents. In the short-term, the goal was to resolve the knee pain and thus enable the patient to resume sports. In the medium-term, the goal was to reduce the genu varum and the scoliotic deformity. In the long-term, the treatment goal was to prevent these conditions from having a functional impact.
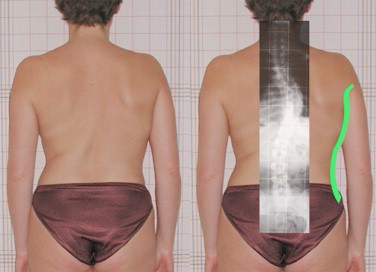
As mentioned above, Postural Reconstruction ® uses “normalizing induction”, a process involving neuromuscular facilitation/inhibition mechanisms ( Fig. 1 ) . Motor irradiation is triggered by high-amplitude, active (or active assisted) movements. Clinical observations show that the irradiation process is likely to amplify remote, pre-existing, spontaneous deformities of the musculoskeletal system located along the irradiation’s pathway. These aggravations are involuntary and cannot be controlled by the patient. The worsening of a pre-existing deformity validates the effect of the normalizing induction manoeuvre. By maintaining the inducing effort, the worsening of the deformity decreases progressively. Once this reduction has occurred, the treatment can be stopped. The presence of a worsening phase appears to be essential for subsequent achievement of the desired corrective effect. A full postural evaluation in all three planes must therefore be performed in all cases, in order to select the deformities that will be transiently worsened. When evaluating the trunk, Nisand suggested that rigorous analysis of morphological contours enables the clinician to infer the shape of the spine in three dimensions . The correlation between the scoliotic curves and the shape of the trunk can be revealed by superimposing photos and X-ray images ( Fig. 2 ). The importance that Nisand attaches to the observation of morphological contours concurs with Bernard’s recommendations on evaluating the thorax’s external contours in scoliosis .
In the present case, we sought to reduce the genu varum and the scoliotic deformity. In Postural Reconstruction ® , these deformities are transiently aggravated during the physiotherapy session. A normalizing induction manoeuvre involving arm abduction was selected for its ability to induce the desired aggravations. Although other induction manoeuvres were applied (albeit much less frequently), only the arm abduction manoeuvre is described here. The normalizing induction was achieved by combining maximal medial rotation of the arm with abduction ( Fig. 3 ). The patient achieved the required maximum medial rotation by performing a 30° elbow flexion and ensuring that his wrist remained in contact with ground. At the end of the movement, the arm forms a smooth curve. This combination of movements almost always induces uncontrolled convexification of the ipsilateral contours of the trunk. The hypothesis is that this convexification reflects the accentuation of the spinal convexity through involuntary activation of the contralateral paraspinal muscles ( Fig. 4 ).
Related posts:
 Is there a place for general journals of rehabilitation?
Executive functions of children with developmental dyspraxia: Assessment combining neuropsychological and ecological tests
A survey of medical and paramedical involvement in children with cerebral palsy in Britanny: Preliminary results
Qualities of a French version of the Wolf Motor Function Test: A multicenter study
Is there a place for general journals of rehabilitation?
Executive functions of children with developmental dyspraxia: Assessment combining neuropsychological and ecological tests
A survey of medical and paramedical involvement in children with cerebral palsy in Britanny: Preliminary results
Qualities of a French version of the Wolf Motor Function Test: A multicenter study
 The piriformis muscle syndrome: An exploration of anatomical context, pathophysiological hypotheses and diagnostic criteria
The piriformis muscle syndrome: An exploration of anatomical context, pathophysiological hypotheses and diagnostic criteria
 Parent–Professional Partnership
Parent–Professional Partnership
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


