Use of Porous Metals and Augments for Acetabular Revision
David Licini
R. Michael Meneghini
Introduction
Significant bone loss can be a tremendous challenge when encountered in acetabular revision. To date, reconstruction of the acetabulum has had great success with cementless, porous-coated cups for the majority (90% to 95%) of acetabular defects. Reliable osseointegration has been demonstrated when viable host bone is in contact with greater than approximately 50% of the porous-coated implant and initial mechanical stability is obtained. This has led to multiple studies reporting excellent survivorship with failure rates for aseptic loosening at less than 5% at 10 years or more (1,2,3,4,5).
When bone loss is so severe that standard hemispherical acetabular components are insufficient, the optimal reconstruction method has not been determined. Traditionally, structural bulk allograft, antiprotrusio cages, and custom implants have been the predominant means of reconstructing severe acetabular bone defects. The midterm results for these complex reconstruction cases have been satisfactory.
Lee et al. (6) reported their experience with structural allografts for uncontained defects involving 30% to 50% of the acetabulum. At 15 and 20 years, the survivorship for aseptic loosening was 67% and 61%, respectively, with a 19% graft resorption rate leading to failure via migration of the cup (6). Antiprotrusio cages have had reasonable results for difficult bone loss, however midterm results have reported failure rates of approximately 15% (7), along with a high rate of complications including sciatic nerve injury, loss of fixation, and fracture of the flanges of the cage (8). Finally, acetabular reconstruction with custom implants have also been shown to be useful but are associated with high rates of complications, excessive cost, and requires a delay in surgery for fabrication of the custom implants (9,10).
The increased burden of revisions in the future and the problems associated with the techniques previously described have served as a stimulus for development of new implants with enhanced biologic and mechanical properties that are surgeon friendly in difficult acetabular bone loss situations. In the late 90s a new generation highly porous tantalum metal acetabular component with a high coefficient of friction and optimal bone ingrowth potential was developed. Soon following was a complimentary augment system to provide adjuvant fixation and support where bulk allograft, custom implants, and cages might otherwise have been used traditionally. The purpose of this chapter is to review these newer generation highly porous metal augments, with regard to biomaterial characteristics and prosthetic design, indications for use, surgical technique, common complications, and discuss the early clinical results.
Case Example
A 70-year-old male presented with a long history of left hip pain with a sudden and acute exacerbation 5 days prior to presentation. The patient’s medical history was complicated because of a failed kidney transplant that necessitated hemodialysis treatments on a regular basis. The patient had previously undergone a primary total hip replacement 20 years ago followed by a subsequent revision of the acetabular component 7 years ago for acetabular component aseptic loosening. On presentation the patient’s physical examination was dramatic with the inability to bear any weight on the left lower extremity, with the hip held in a flexed, adducted and shortened position with extreme pain during attempted motion. Radiographs demonstrated a dislocated revision total hip arthroplasty with a well-fixed cementless femoral component (Fig. 110.1A). The acetabular component was a revision-type porous tantalum shell with a posterosuperior wedge augment. The acetabular component was positioned vertically and laterally with a zone 3 gap consistent with loosening. ESR and C-reactive protein were markedly elevated and hip aspiration revealed gross purulent fluid with an elevated white blood cell count consistent with deep periprosthetic infection. The patient was taken to the operating room and a resection total hip arthroplasty with insertion of antibiotic-impregnated articulating cement spacer was performed (Fig. 110.1B). At the time of surgery, the acetabulum was found to have severe posterior-superior acetabular bone loss, yet with a contained peripheral cortical supporting rim. The anterior and posterior columns were intact and enacted
a hemispherical shape with approximately 40% of the superior hemisphere uncovered because of the bone deficiency in the posterior ilium and superior-posterior column.
a hemispherical shape with approximately 40% of the superior hemisphere uncovered because of the bone deficiency in the posterior ilium and superior-posterior column.
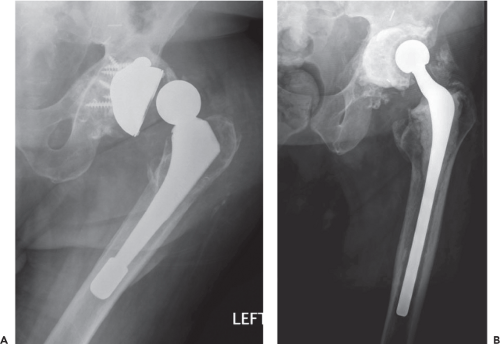 Figure 110.1. A: Anteroposterior radiograph of failed left total hip arthroplasty secondary to chronic periprosthetic infection and instability. B: Postoperative anteroposterior radiograph demonstrating the high-dose antibiotic-laden articulating cement spacer. |
Biomaterial Characteristics and Prosthetic Designs
Essential to the clinical results of newer generation highly porous metal implants is the porosity. The porosity of the majority of commercially available implants is 75% to 85% and exceeds that of previous first- and second-generation porous-coated implants. This property allows for a higher fractional volume available for ingrowth and leads to more rapid development of interfacial shear strength (11,12). A 4-week histologic analysis study of highly porous tantalum determined superior bone ingrowth (40% to 50%) and interface fixation strength compared to previous less volumetric porous-coated materials (12).
The wedge-shaped augments are the workhorse of highly porous metal revision acetabular systems, whether porous tantalum or porous titanium. These augments come in various shapes and sizes and give the surgeon the ability to address bone loss of varying extents. The goal of the augments is to not only provide initial mechanical stability to the shell but to provide a scaffold for bone ingrowth to occur. The augments can be used anywhere in the acetabulum where deemed appropriate and avoid the need for structural bone grafting (13). The augments are wedge shaped and contain screw holes for fixation to the host bone. In addition, some augment systems are equipped with small K-wire holes for provisional fixation of the trial implant that facilitates reproducible positioning of the final implant during screw fixation to host bone (Fig. 110.2A–C).
Indications and Preoperative Planning
For the vast majority of cases, a traditional porous-coated cementless acetabular component can be used with excellent success. The indications for use of modular augments in acetabular reconstruction are similar to those for traditional bulk allograft, bilobed implants, and triflange components. Although there is little research, typically a lack of 40% to 50% viable host bone is considered an inadequate amount of viable host bone contact to provide sufficient mechanical stability and the appropriate biologic conditions to allow bone ingrowth and long-term clinical success with a porous-coated shell alone. Common examples where modular augments may be indicated include large irregular acetabular defects and/or small acetabular anteroposterior (AP) dimensions that render a hemispheric cup unstable, major segmental defect in the dome or posterior column and pelvic discontinuity.
Defect Classification and Augment Reconstruction Strategy
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


