21 Upper limb
Cases relevant to this chapter
Essential facts
1. In rotator cuff disease it is important to discriminate between inflammation and tear in the younger patient. Local anaesthetic injection and ultrasonography will help achieve a diagnosis.
2. Frozen shoulder is a self-limiting condition in middle-aged and older adults.
3. Dupuytren’s disease is characterized by thickening and shortening of the longitudinal fibres of the palmar and digital fascia.
4. Trigger finger is more common in people with diabetes or rheumatoid arthritis (RA).
5. The most common sites for hand osteoarthritis are the trapezio-metacarpal joint of the thumb ray and the distal interphalangeal joints.
6. In RA, inflammatory synovitis causes stretching of the capsules of the small joints of the hand and damage to tendons, producing characteristic problems of ulnar deviation, thumb deformities and tendon ruptures.
7. Carpal tunnel syndrome is common; tingling, pain and numbness are much more troublesome at night.
Shoulder
Impingement syndrome and rotator cuff disease
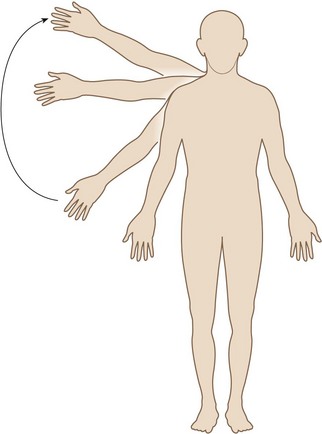
Movement of the shoulder in rotation and initiation of abduction is produced by action of the rotator cuff – a conjoined tendon that is also a roof to the gleno-humeral joint capsule described in Chapter 1. When the shoulder abducts, the tendon has to be accommodated underneath the acromion. This may result in impingement between the acromion and the cuff where it inserts into the greater tuberosity. Usually the subacromial bursa will act as a buffer to prevent a frictional reaction, but in middle age there is a tendency for inflammation to occur within the bursa after shoulder exercise. If only the bursa and cuff are inflamed, this is known as (subacromial) impingement syndrome. It is painful to elevate and abduct the arm through an arc of movement of about 45–120° (Fig. 21.1). There may be only slight tenderness just lateral to the acromion, but special tests for impingement are usually positive (Jobe’s test puts the greater tuberosity under the acromion in shoulder abduction and internal rotation; forced abduction against resistance now provokes pain). Resolution may be expected, but can be speeded by steroid injection into the subacromial bursa. Plain radiographs may reveal acute calcification (calcific tendonitis) within the supraspinatus tendon; if acute, then chalky material may be aspirated, providing instant relief. Where plain radiographs show osteophytic ‘beaking’ of the lateral edge of the acromion or a reduced distance between the humerus and the acromion, steroid injection may help but will not provide a cure. Arthroscopic subacromial decompression of the bony spur and debridement of inflammatory soft tissue may give relief. A tear of the rotator cuff may be partial or complete. A tear of any size may inhibit abduction through pain, so a diagnostic local anaesthetic injection into the subacromial bursa, followed by assessment of active movement, may be diagnostic of the extent of a tear. Ultrasonography or magnetic resonance imaging (MRI) can define its extent further. A small tear can be managed as impingement syndrome. A medium-sized tear can be repaired by open or arthroscopic surgery. A chronic massive tear in the elderly is rarely repairable; over time it will result in abnormal forces applied across the gleno-humeral joint and secondary osteoarthritis (cuff arthropathy) will result.
< div class='tao-gold-member'>






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


