Unstable Ulnar Styloid Fracture
22.1 Introduction
The carpus and the radial bone pivot around the distal ulna during rotational movements of the forearm and hand. The ulnar styloid and its immediate vicinity constitute the origin of the ligaments aiding in the congruency of these movements. Therefore, addressing injuries of the ulnar styloid means addressing injuries to the triangular fibrocartilage complex (TFCC).
22.2 Soft Tissue Connections around the Ulnar Styloid
The stability of the hand and distal radius vis-à-vis the distal ulna is not only dependent on the TFCC. The adjacent muscles and tendons (especially the extensor carpi ulnaris [ECU] and pronator quadratus [PQ]) and the distal radioulnar (DRU) joint congruency also contribute. These factors may be more important than the TFCC.
The TFCC confluences around the ulnar styloid and ulnocarpal stabilizers insert upon ligaments responsible for radioulnar stability (▶ Fig. 22.1). Recent studies show that the position of the axis of forearm rotation shifts during rotation and also that the position varies between individuals. Accordingly, the stabilizing effect of the TFCC on distal radioulnar and ulnocarpal stability may be more pronounced in some individuals than in others.
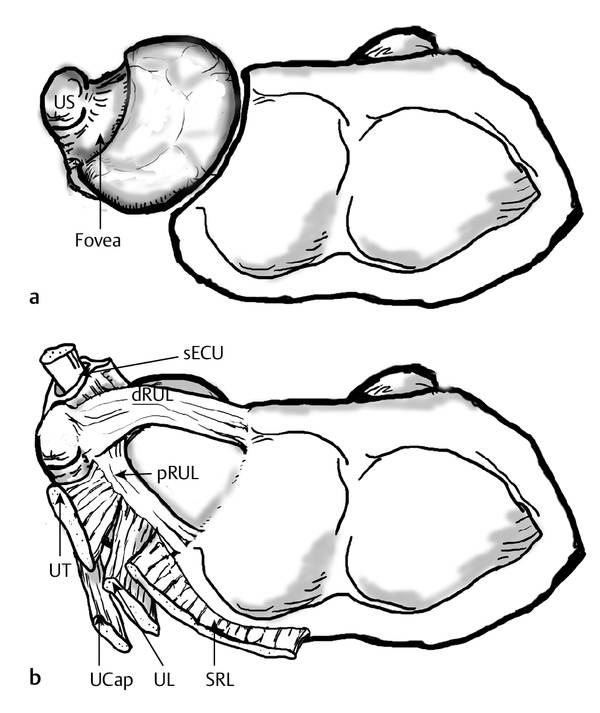
Fig. 22.1 (a and b) The DRU joint and TFCC of the right wrist seen from a distal viewpoint. (a) Bold arrow: fovea of the ulnar head. US, ulnar styloid. (b) The TFCC. sECU, ECU subsheath (with tendon); dRUL, dorsal radioulnar ligament; pRUL; palmar radioulnar ligament; UT, ulnotriquetral ligament; UL, ulnolunate ligament. Also included in the image: SRL, short radiolunate ligament; UCap, ulnocapitate ligament. (Reproduced with kind permission from Johan Scheer, Periulnar Injuries Associated with Distal Radius Fractures, Linköping University Medical Dissertations No. 1236, 2011.) (Illustrator: J Scheer.)
22.2.1 Radioulnar Stability
Much has been written on the role of the TFCC in radioulnar stability. The deep dorsal and palmar radioulnar ligaments inserting into the fovea of the ulna, just radial to the ulnar styloid (▶ Fig. 22.1), are the principal ligamentous radioulnar stabilizers together with the interosseous membrane, especially the distal oblique band (DOB), which is present in only 80% of individuals.
22.2.2 Ulnocarpal Stability
Ulnocarpal stability is much less studied. On the palmar side there are the ulnotriquetral (UT) and ulnolunate (UL) ligaments both of which originate on the palmar radioulnar ligament and are considered a part of the TFCC (▶ Fig. 22.1). There is also the extrinsic ulnocapitate (UC) ligament that runs from the base of the ulnar styloid to the capitate. All these structures become taut in supination of the forearm, in dorsiflexion, and in radial deviation of the carpus
On the dorsal side, the floor of the ECU tendon sheath is attached both to the distal ulna and to the TFCC. Separation between the subsheath and the dorsal radioulnar ligament (dRUL) results in a palmar displacement of the ulnar carpus in pronation.
22.3 Classification of Ulnar Styloid Fractures
A good classification aids understanding of injuries and guides treatment. Ulnar styloid fractures are avulsion fractures due to pulling of the ligaments inserting about the styloid: both location and displacement have to be taken into consideration. We use a definition of a base fracture as a reference, since no components of the TFCC insert proximal to the fovea (▶ Fig. 22.2). In minimally displaced fractures the TFCC may be intact, but elasticity of the ligaments cannot permit more than 2 mm of displacement without rupture.
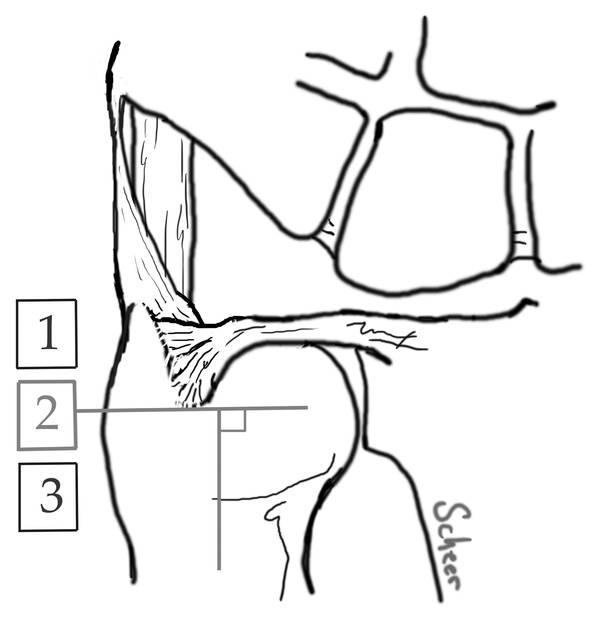
Fig. 22.2 Classification of ulnar styloid fractures, palmar view. Type 1: Distal to the base where superficial fibers of the TFCC insert as well as the dorsal UT ligament (Sasao et al3). Type 2: Base fracture: goes through a line perpendicular to the ulnar shaft and into the proximal limitation of the fovea, but does not involve the articular surface of the ulnar head. Type 3: Proximal to a type 2 fracture. (Reprinted from Scheer, Johan H., Adolfsson, Lars E. Patterns of triangular fibrocartilage complex (TFCC) injury associated with severely dorsally displaced extra-articular distal radius fractures. Injury 2012: 43(6): 926–932 with permission from Elsevier.2)
22.4 Patterns of Injury
A fall on the palm of the hand is most commonly responsible for ulnar styloid/TFCC injuries. The displacing forces from the hand can be absorbed both through the radial and through the ulnar side of the carpus and forearm. The propagation of forces to the TFCC can take two possible routes. One is through the radius, resulting in tensile forces of the radioulnar (pRUL and dRUL) ligaments. The other is by tensioning of the ulnocarpal ligaments, which insert upon the pRUL and dRUL. It is important to remember that injuries of both the ulnocarpal and radioulnar stabilizers can coexist.
22.4.1 Ulnar Styloid Fractures with an Associated Distal Radius Fracture
The individual sequence of events is unknown. It is evident that in cases of severe distal radius fragment displacement large strain is developed in the ulnocarpal ligaments as the carpus follows the distal radius. It can also be noted that displacement during the injury is probably more pronounced than is seen on initial radiographs.
Two specific injury patterns of extra-articular dorsal displacement have been observed both in a cadaveric model and in patients.1,2 Other patterns may be possible in intra-articular fractures or in minimally displaced fractures. However, it is important to realize that ulnocarpal injuries (especially ECU subsheath injuries) can exist in isolation or concurrently with a deep foveal injury. The latter can also show a progression when the forces continue to peel the TFCC off the ulnar head.
Type 2 Ulnar Styloid (Base) Fracture (▶ Fig. 22.3)
The distribution of forces in the TFCC bends the whole ulnar styloid. First it snaps off in the base with the ligaments intact, then with further displacement the entire TFCC is peeled off from the fovea together with the styloid.1 Thus, with repair of the styloid fracture the TFCC is simultaneously restored to its origin.

Fig. 22.3 TFCC lesion with a type 2 ulnar styloid fracture. Arrows: pull of palmar ulnocarpal ligaments. Dorsopalmar view, right wrist. Tr, triquetrum; UT, ulnotriquetral ligament, UCap, ulnocapitate ligament; ECU, extensor carpi ulnaris. (Reproduced with kind permission from Johan Scheer, Periulnar Injuries Associated with Distal Radius Fractures, Linköping University Medical Dissertations No. 1236, 2011.)
Type 1 Ulnar Styloid (Tip) Fracture (▶ Fig. 22.4)
The ulnar styloid fragment is not attached to the TFCC components described previously (▶ Fig. 22.4); instead, it appears to be attached to fibers running between the ulnar styloid and triquetrum.3 The first step of the TFCC injury is probably a separation of the deep layers of the ECU tendon sheath from the dRUL followed by a foveal injury of the radioulnar attachments.1,2 Therefore, a complete repair can imply both a foveal reinsertion and a subsheath repair.
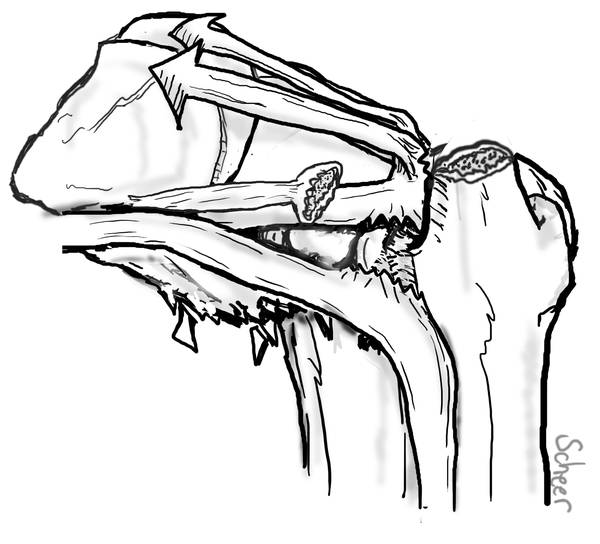
Fig. 22.4 TFCC lesion with a type 1 ulnar styloid fracture. Arrows: Pull of ulnocarpal ligaments. Dorsopalmar view, right wrist. Tr, triquetrum; dRUL, dorsal radioulnar ligament; UT, ulnotriquetral ligament; UL, ulnolunate ligament; ECU, extensor carpi ulnaris. (Reproduced with kind permission from Johan Scheer. Periulnar Injuries Associated with Distal Radius Fractures, Linköping University Medical Dissertations No. 1236, 2011.)
22.4.2 Ulnar Styloid Fractures without an Associated Distal Radius Fracture
Ulnar styloid fractures are less common in TFCC injuries without an associated distal radius fracture, and the ones that occur are usually type 1 fractures.4 Pulling of ulnocarpal ligaments can be involved, but possibly a higher degree of rotational force vectors is evoked and a correspondingly higher strain in the dRUL and/or pRUL results in different injury patterns.4 Our observation is that in displaced fractures, an sECU injury is always present, in undislplaced it might be present or it might not be.
22.4.3 Galeazzi Fractures
Not all isolated radial shaft fractures are associated with TFCC injuries. Ulnar styloid fractures are usually type 2 fractures.5
22.5 Diagnostics
The ulnar styloid fracture is obviously visible on plain radiographs—it is the associated soft tissue injury that is harder to assess.
22.5.1 Clinical Assessment
Acute Setting
Wrist trauma followed by swelling and tenderness around the distal ulna is suggestive of an injury. A radioulnar laxity test of the radioulnar connections can be performed unless an unstable distal radius fracture is present, making it hard to stabilize the radius to the carpus. Pain may further obscure laxity testing.
The radioulnar laxity test is performed by stabilizing the radius to the carpus with one hand and displacing the distal ulna with the other, comparing with the contralateral side. Pathological laxity is noted in the absence of a firm end-feel.6
Chronic Setting
Pain on palpation is usually present around the distal ulna. This can be due to local synovitis or an underlying pseudarthrosis. Radioulnar laxity testing shows good inter-rater reliability.7 If the radioulnar ligamentous connections are intact, an isolated ECU subsheath injury is often revealed in pronation; indeed, in that position the carpus can be seen protruding palmarly, subluxated in relation to the ulna compared to the other side. Patient relief can be appreciated by pressing pisiform dorsally in this position.
22.5.2 Radiographic Assessment
Computed tomography (CT) has little or no role in identifying TFCC injuries,6 but it can be used as a complement to plain radiographs when elucidating bony anatomy. If MRI is used, high resolution with thin slices is recommended.8
22.6 Indications for Acute Repair of Ulnar Styloid Fractures
The argument for acute repair is compelling because the newly injured raw surfaces probably provide a good bed for healing. We consider this window of opportunity to be within 6 to 8 weeks of injury. There is, however, little evidence supporting acute repair of all patients with ulnar styloid fracture/TFCC injury. On the contrary, in an adult population few patients with a well-reduced distal radius fracture experience substantial effect on wrist function.9–11
Related posts:
 Undisplaced Scaphoid Fractures
Undisplaced Scaphoid Fractures
 Proximal Row Fractures (Other Than Scaphoid and Pisiform Fractures): Triquetrum and Lunate Fractures
Proximal Row Fractures (Other Than Scaphoid and Pisiform Fractures): Triquetrum and Lunate Fractures
 Intra-articular Fractures of the Distal Radius (AO types C3, with Special Focus in C3.3), Open Approach
Intra-articular Fractures of the Distal Radius (AO types C3, with Special Focus in C3.3), Open Approach
 Fracture-dislocations Other than Perilunate
Fracture-dislocations Other than Perilunate
 Intra-articular Fractures of the Distal Radius (AO type C3), (Dry) Arthroscopic Approach
Intra-articular Fractures of the Distal Radius (AO type C3), (Dry) Arthroscopic Approach
 Role of Hand Therapy in the Treatment of Wrist Instability
Role of Hand Therapy in the Treatment of Wrist Instability
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


