CHAPTER 11 Unicompartmental Knee Arthroplasty
Mobile-Bearing Techniques
 The Oxford mobile-bearing unicompartmental knee arthroplasty is indicated for anteromedial osteoarthritis with an intact anterior cruciate ligament.
The Oxford mobile-bearing unicompartmental knee arthroplasty is indicated for anteromedial osteoarthritis with an intact anterior cruciate ligament.


Introduction
Anteromedial arthritis of the knee with an intact anterior cruciate ligament, as described by White et al., is a distinct pattern of osteoarthritis that is appropriately treated with unicompartmental arthroplasty when conservative measures fail.1 Unicompartmental knee arthroplasty for anteromedial osteoarthritis with a functional anterior cruciate ligament utilizing a mobile meniscal polyethylene bearing (Oxford Unicompartmental Knee Arthroplasty, Oxford, UK) has demonstrated 92.3% survivorship at 20 years.2 Clinical results have been good or excellent in 91% of patients at minimum 10-year follow-up utilizing Hospital for Special Surgery Knee Scores.3 Wear rates of the polyethylene have been reported as 0.01 mm/year when the device is functionally normally without intra-articular or extra-articular impingement.4 Rapid recovery protocol utilization has resulted in faster functional return than with total knee arthroplasty.5 There remains concern regarding the increased difficulty in performing this operation, and early failures are often due to technical errors. New instrumentation has been developed (Oxford Microplasty Instrumentation; Biomet, Warsaw, IN) that allows more predictable execution of the procedure while minimizing technical errors. The enhanced performance of the operation should further improve the previously reported excellent clinical and survivorship successes of this mobile-bearing unicompartmental knee arthroplasty.
Setup and Equipment
A tourniquet should be placed on the proximal thigh of the operative limb. A hanging leg holder is utilized to have the operative extremity flexed 30° at the hip with enough abduction to allow at least 135° of knee flexion without impingement on the operative table (Fig. 11–1). The contralateral leg is placed in a well-padded foam leg holder. The foot of the bed is dropped perpendicular to the floor. A stiff, narrow reciprocating saw, a 12-mm-wide oscillating saw, and a double-armed vertical toothbrush saw are utilized during the operation (Fig. 11–2) (Oxford Knee Resection Procedure Three Pack; Synvasive Technologies Inc., El Dorado Hills, CA). A Woodson-style curette is an excellent cement removal tool. Standard knee retractors and instruments are used. Radiographs are reviewed for anteromedial arthritis and appropriate restoration of the knee with valgus stress radiograph (Fig. 11–3A-D). Preoperative templating of the femoral component size is performed using the lateral radiograph (Fig. 11–3E).




Approach
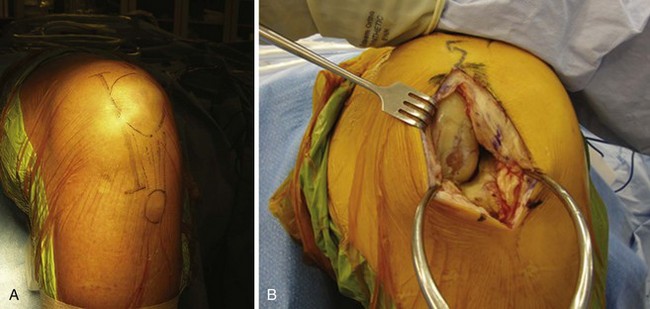
The operative extremity is exsanguinated and the tourniquet is insufflated to 350 mm Hg. The knee is allowed to flex 90° with gravity in the hanging leg holder. A slightly oblique skin incision is made from the superomedial edge of the patella to a point 3 cm inferior to the joint line, medial to the tibial tubercle (Fig. 11–4A). An arthrotomy is performed with proximal extension of 1–2 cm into the vastus medialis at the level of the superomedial pole of the patella (Fig. 11–4B). Electrocautery is used to expose the anteromedial aspect of the tibia to allow for later positioning and visualization of the tibial resection guide. None of the medial collateral ligament is released. The anterior horn of the medial meniscus is excised. A small portion of the retropatellar fat pad is excised to allow visualization of the anterior cruciate ligament and the lateral compartment of the knee (Fig. 11–5). If the anterior cruciate ligament is nonfunctional or there is full-thickness lateral compartment osteoarthritis upon inspection, conversion to a total knee arthroplasty is undertaken.
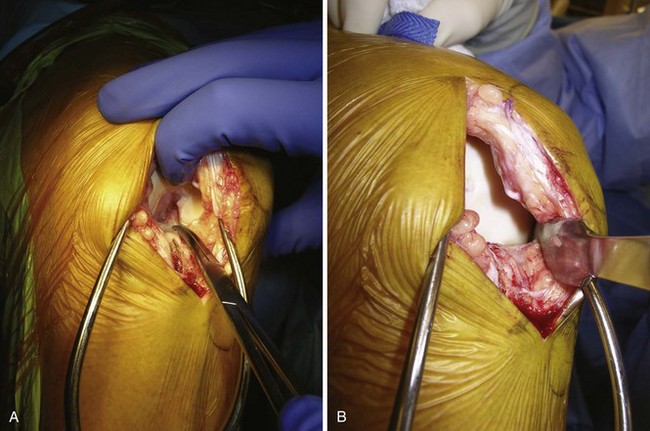
Assuming the anterior cruciate ligament and the lateral compartment are normal, the unicompartmental arthroplasty continues. Osteophytes are removed with an osteotome from the medial and lateral aspects of the intercondylar notch as well as from the medial margin of the medial femoral condyle. A small rongeur is used to remove the anvil osteophyte anterior to the anterior cruciate ligament insertion on the tibia. The anteromedial osteophyte on the tibia is removed and the blush of bleeding bone from its removal serves as a guide for depth of resection for the tibial osteotomy (Fig. 11–6).
< div class='tao-gold-member'>

Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


