Treatment of large segmental defects using conventional autogenous iliac crest bone graft can be limited by volume of cancellous bone and donor site morbidity. The reamer-irrigator-aspirator (RIA) technique allows access to a large volume of cancellous bone graft containing growth factors with potency equal to or greater than autograft material from the iliac crest. The purpose of this study was to evaluate the effectiveness of RIA-harvested autogenous bone graft for treating large segmental defects of long bones.
Treatment of large segmental bone defects is a difficult challenge for orthopedic surgeons. These large defects can be caused by traumatic injury or surgical treatment of infection or tumors. Historically, amputation was the best option for many of these patients, but limb salvage has become more common. Review of available literature demonstrates that several treatment modalities have had some success in treating segmental bone defects:
Ilizarov bone transport
Autogenous cortical or cancellous bone graft
Vascularized fibula graft
Recombinant bone morphogenic protein
Calcium phosphate fillers
Autogenous bone graft has been the gold standard for bone graft. It is osteogenic, osteoinductive, and osteoconductive. When the defect is large, however, the traditional supply of autogenous graft may not be sufficient. There can be significant morbidity with harvesting large quantities of bone. Many studies show high incidences of complications from iliac crest harvest, including donor site pain and injury to cutaneous nerves resulting in painful neuromas. With the recent availability of bone morphogenic protein (BMPs), many surgeons have decreased their use of autogenous bone graft to avoid potential complications at the donor site. Although there are several studies that show BMP is effective for nonunions and healing cortical defects, its high cost may be prohibitive at some institutions, especially in very large defects, where a large quantity of graft would be needed.
Bone grafting of defects often is delayed after primary internal fixation to allow soft tissue healing, decrease infection risk, and prevent graft resorption during the early inflammatory healing phase. Cement spacers with antibiotics can be used to temporarily fill defects. This has many advantages. Cement can give structural support and decrease implant loading. It maintains a void that allows easy placement of graft and provides local antibiotics in areas of open fractures at high risk for infection. Cement spacers also induce formation of pseudosynovial membrane, which creates a contained defect for bone grafting. This membrane has been shown to produce growth factors and osteoinductive factors including BMP-2.
The reamer-irrigator-aspirator (RIA) originally was designed as a single-pass intramedullary reamer that creates a negative pressure within the canal in an effort to decrease pulmonary insult from marrow contents during the course of reaming for femur fractures. RIA has several unique characteristics allowing it to achieve this result. The reamer head is extremely sharp. It is a single-use reamer that allows reaming to a premeasured diameter with a single pass, as opposed to sequential passes with incrementally larger reamers. It also has both an irrigation and aspiration port. Irrigation of the canal with normal saline during the reaming process decreases the overall temperature within the canal and assists in the aspiration process, as it decreases the viscosity of the intramedullary contents. Aspiration allows for removal of reaming debris and creates constant negative pressure in the canal. RIA has been used to debride the intramedullary canal for treatment of bone infections. It also can be modified by placing a screen trap in line with the aspiration port to capture the bone debris aspirated from the medullary canal in a sterile fashion.
The ideal treatment for large segmental defects of long bones would be inexpensive, have minimal adverse effects, be effective at obtaining union, and provide enough graft volume to fill the defect. The intramedullary canal of femurs and tibias is relatively easy to access and contains large amounts of cancellous bone graft. Intramedullary reamings have been shown to have viable cells capable of new osteosynthesis. Recent quantitative analysis found higher levels of fibroblast growth factor (FGFa), platelet-derived growth factor (PDGF), insulinlike growth factor (IGF)-1, BMP-2, and transforming growth factor (TGF)-β1 in RIA bone graft compared with iliac crest bone graft. This study is designed to evaluate the efficacy of healing and associated complications in patients with large segmental defects treated with bone graft obtained by RIA.
Materials and methods
This prospective study was conducted between February 2003 and March 2007. Investigators obtained institutional review board approval and written informed consent from all patients. Twenty one patients, 13 male and 8 female, with an average age of 30.6 years, with segmental bone defects agreed to participate. The defect size ranged from 2 to 14.5 cm (average 6.6 cm). Three patients had at least one surgical procedure at an outside hospital. All subsequent surgeries were performed by fellowship-trained orthopedic trauma surgeons at a level 1 trauma center. Eight patients smoked, and 13 did not. Mechanism of injury included nine motorcycle collisions, five motor vehicle collisions, four gun shot wounds, one car versus pedestrian, one car versus bicyclist, and one crush injury. There were 5 femurs, 15 tibias and 1 ulna treated. The average time from initial injury to RIA procedure was 141 days (range 31 to 582 days).
All patients with open fractures were treated with appropriate surgical debridements and antibiotics. Box 1 outlines the treatment algorithm. An average of 4.8 procedures were performed at the defect site before placement of bone graft. The 20 open fractures were classified as 8 grade 3A, 9 grade 3B, and 2 grade 3C. Eight patients needed soft tissue flap coverage, including three free flaps and five local flaps. Eighteen patients had antibiotic spacers placed into the defect site before bone grafting. The RIA graft was obtained from 21 femurs and 2 tibias. One patient had bone graft harvested from both the contralateral tibia and femur, and another had bone harvested from the ipsilateral femur and contralateral tibia. Filtered bone graft volume was measured in 19 patients. The amount of bone graft harvested was not maximized in patients with smaller defects.
Open Fractures
Antibiotics in emergency room
Urgent irrigation and debridements (I&D) in operating room with removal of devascularized soft tissue and bone
Internal or External Fixation
Plus or minus VAC dressing
Repeat I&Ds until wound clean and all devitalized tissue removed
Definitive fixation with plate or nail if previously ex fixed
Wound closed or covered with flap
Antibiotic cement spacer placed into defect
Incisions and soft tissues allowed to heal (4 to 6 weeks)
Psuedomembrane incised and cement spacer removed
Fibrous tissue debrided from defect if polymethylmethacrylate (PMMA) spacer not used
Medullary canal opened
Defect grafted with RIA bone graft if no sign of infection
Weight bearing limited until radiographic consolidation
Surgical Technique
After induction of general anesthesia, the patients were positioned supine on a radiolucent table. The defect site was prepared first to ensure that there was no sign of infection and to limit the time span that the graft was exposed out of the body. An appropriate skin incision was made depending on location of the defect and previous incisions. In cases with PMMA spacers, the pseudomembrane enveloping the spacer was incised longitudinally to allow for closure after grafting. The spacer was removed and the bone edges cleaned of interposed fibrous tissue.
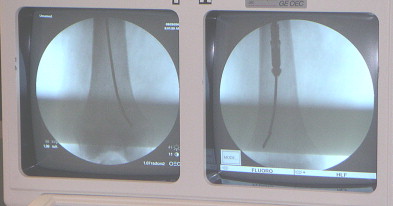
When graft was harvested from the femur, a bump was placed under the ipsilateral pelvis similar to position for free leg femoral nail. The narrowest section of the femur or tibia was templated on anterior–posterior (AP) and lateral fluoroscopy to determine the intramedullary canal size ( Fig. 1 ). Reamer size then was chosen to be approximately 1 to 1.5 mm larger than the determined canal size. A percutaneous technique was used to locate the piriformis fossa or lateral starting point at the tip of the greater trochanter. This was verified with biplanar fluoroscopy. The standard entry point for tibial intramedullary nailing was used for tibial graft harvest. A 13 mm cannulated drill bit was used to open the entry site, after which a ball tip guide rod was advanced down the canal. The Reamer Irrigator Aspirator (RIA) system (Synthes, West Chester, Pennsylvania) then was prepared to harvest bone graft ( Fig. 2 ). This included attaching an appropriately sized reamer head, a 3 or 5 L saline bag to the irrigation port, suction to the aspiration port and a screen trap in line with the suction tubing. The Screen Trap (Biomet, Warsaw, Indiana) has a pore size of approximately 500 μm. Gravity flow and vacuum suction were used to maintain irrigation flow. The canal then was reamed with an appropriately sized reamer in an alternating advance-and-withdraw motion (see Fig. 1 ). The femur received two to four passes of the RIA. For larger defects, graft volume can be increased by positioning the guide rod in the lateral condyle first and then into the medial condyle to enable graft acquisition from both ( Fig. 3 ). When reaming is completed, the trap is disconnected and bone graft collected. The harvested bone graft then is packed into the defect. The pseudomembrane is closed to contain the graft, and skin incisions are closed.
Results
Follow-up
Twenty of the 21 patients (95%) have been followed to conclusion. Patients were followed clinically and radiographically until declared healed or failure of treatment. One patient (5%) was lost to follow-up before complete healing.
Graft Harvest
The bone graft volume was measured in 19 of the 21 patients and averaged 64 cc. Two patients had graft harvested from a femur and a tibia. As expected, tibia bone graft volume (37.5 cc) was less than femur volume (67 cc). These extracted volumes, however, were not the maximum volume of graft available. Patients with smaller defects needed less bone graft; therefore less graft was harvested.
Donor Site Complications
No patients had serious donor site morbidity. There were no donor site hematomas, infections, or fractures. No second surgeries were required at donor sites. The authors did not perform routine radiographic examinations of donor bone site. Eight patients who had antegrade femoral RIA procedures had pelvis or hip radiographs for follow-up of pelvic ring or contralateral hip injuries. Two of these patients (25%) were noted to have Brooker class 1 heterotopic ossification in the soft tissues near the abductor insertion. None of these patients had clinical or subjective symptoms at donor site.
Defect Site Complications
Of the 20 patients followed to conclusion, 10 had no defect site complications after bone grafting. Ten patients (50%) had defect site complications. There were six deep infections and four nonunions (two with hardware failure). Four of the patients with infection and three with nonunion eventually healed the defect.
Defect healing
Twenty patients with segmental bone defects were followed to conclusion. There were 5 femurs, 14 tibias, and 1 ulna. Eighteen of these 20 patients had PMMA spacers in the defect before bone grafting. Sixteen patients were treated with plates, and 4 were treated with intramedullary (IM) nails. Seventeen of 20 patients (85%) completely healed at an average 11 months (range 2.5 to 39 months). Ten of these 17 (58%) healed with no additional surgery after RIA bone graft. Seven patients needed additional surgeries after original RIA. Two patients healed after exchange intramedullary nail; one patient developed a deep infection but healed after I&D and repeat RIA. One proximal tibia healed after revision compression plating with cancellous bone graft harvested from the distal femur, and one healed after I&D and Enders rod (West Chester, Pennsylvania) placement. One healed after repeat I&Ds, and one developed deep infection after the defect healed, requiring I&D and plate removal ( Table 1 ).
| Outcome | N | Comments |
|---|---|---|
| Healed without further surgery | 10 | No further surgery after RIA |
| Healed with further surgery | 7 |
|
| Failed | 3 |
|
Illustrative Case (1st RIA Case Performed)
A 35-year-old woman presented 6 months after a motorcycle accident with a large, open, draining wound of her tibia. After debridement of the wound and bone, she had a 14 cm defect that was managed with a block of methylmethacrylate and covered with a free flap ( Fig. 4 ). Eight weeks later with a stable wound, the RIA was used to harvest bone graft from the ipsilateral femur using a piriformis entry site. The bone graft was used to fill the 14 cm defect with no adjunctive materials added. Ultimately, the patient went on to union of the defect at about 10 months after bone grafting. Hardware removal was performed because of prominent hardware that was causing pain. Unfortunately, the patient fractured through the graft while snow skiing and required a replating. An attempt was made at union with casting. At the time of replating the patient did not have any formal bone grafting other than some local bone graft taken from prominent bone where the bone had grown up around the previously removed plate. Her final radiographs after replating show solid union ( Figs. 5–8 ) of the tibia and recovery of the donor femur site.
Related posts:
 Use of Solid and Cancellous Autologous Bone Graft for Fractures and Nonunions
Use of Solid and Cancellous Autologous Bone Graft for Fractures and Nonunions
 Autologous Bone Graft: When Shall We Add Growth Factors?
Autologous Bone Graft: When Shall We Add Growth Factors?
 Quantitative Analysis of Growth Factors from a Second Filter Using the Reamer-Irrigator-Aspirator System: Description of a Novel Technique
Quantitative Analysis of Growth Factors from a Second Filter Using the Reamer-Irrigator-Aspirator System: Description of a Novel Technique
 Clinical Use of Resorbable Polymeric Membranes in the Treatment of Bone Defects
RIA: One Community’s Experience
Clinical Use of Resorbable Polymeric Membranes in the Treatment of Bone Defects
RIA: One Community’s Experience
 Quantitative Analysis of Growth Factors from a Second Filter Using the Reamer-Irrigator-Aspirator System: Description of a Novel Technique
Quantitative Analysis of Growth Factors from a Second Filter Using the Reamer-Irrigator-Aspirator System: Description of a Novel Technique
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


