Treatment of Enchondroma, Bone Cyst, and Giant Cell Tumor of the Distal Upper Extremity
Edward A. Athanasian
DEFINITION
Enchondromas are benign cartilaginous neoplasms that are commonly seen in the medullary cavity of phalanges and metacarpals and less commonly in the radius and ulna. Enchondroma is the most common neoplasm of bone arising in the hand.
Unicameral bone cysts are benign endothelial-lined fluid-filled cavities arising in metaphyseal bone; they are occasionally seen in the distal radius and rarely seen in the hand.
Giant cell tumor of bone is an uncommon neoplasm of bone, which is locally aggressive and can metastasize. Although its histology suggests a benign process, is behaves as a lowgrade malignancy.
ANATOMY
Enchondroma most commonly arises in the proximal phalanx or metacarpal when seen in the hand (FIG 1A). It can be seen in metaphyseal and epiphyseal regions and is typically confined to the bone. The enchondroma may distend the bone and pathologic fracture may be seen.
Unicameral bone cysts are rarely seen in the hand. When presenting in the radius, they are often metaphyseal and may be in continuity with the distal radial physis (FIG 1B). Unicameral bone cysts are typically confined to bone and pathologic fracture may be seen.
Giant cell tumor of bone most commonly arises in the epiphyseal region except in the skeletally immature patient, in whom it may arise in the metaphysis. The distal radius is the third most frequent location for these tumors (FIG 1C), after the distal femur and the proximal tibia. Hand lesions account for 2% of giant cell tumors of bone.
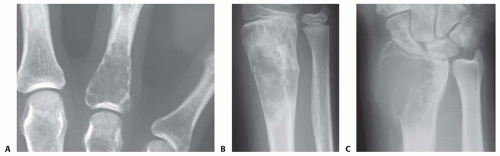 FIG 1 • A. Enchondroma of the proximal phalanx. B. Unicameral bone cyst of the distal radius. C. Giant cell tumor of the distal radius. |
PATHOGENESIS
The pathogenesis of enchondroma, unicameral bone cyst, and giant cell tumor of bone is uncertain. Enchondroma and unicameral bone cysts may be associated with bone development and growth.
Enchondroma, unicameral bone cyst, and giant cell tumor of bone can weaken the bone and predispose the patient to pathologic fracture.
NATURAL HISTORY
Enchondromas are most commonly identified incidentally during unrelated evaluation. They also can present after pathologic fracture. On occasion, a patient may complain of painful swelling in the bone.
Enchondromas found incidentally and not causing considerable mechanical weakness may be observed if typical radiographic findings are seen.
Enchondromas causing substantial fracture risk and those presenting after pathologic fracture can be treated surgically with a low risk of recurrence.7
Enchondromas can extremely rarely transform to chondrosarcomas.
Unicameral bone cysts are most commonly seen during adolescence or childhood. They are most commonly identified after pathologic fracture. Proximal humerus lesions may be seen.
Unicameral bone cysts with a low risk of fracture may be observed with activity modification.
Unicameral bone cysts causing substantial weakness and fracture risk may be treated with surgery or injection.
Suspected unicameral bone cysts in the bones of the hand are sufficiently rare that strong consideration should be given to biopsy when this lesion is suspected.
Giant cell tumor of bone is locally aggressive. Patients may present with pain and swelling or after pathologic fracture.
Giant cell tumor of bone metastasizes 2% to 10% of the time, with metastasis more frequently seen with distal radius and hand lesions.1,2,4,5,6 Metastasis most frequently occurs concurrent with or after a local recurrence.
Patients with giant cell tumor of bone require systemic staging, treatment, and long-term surveillance, as recurrence may be seen late.
PATIENT HISTORY AND PHYSICAL FINDINGS
Enchondroma is most often an incidental finding and is asymptomatic. Pain and deformity can be seen after pathologic fracture. On occasion, there will be bone distention and tenderness with palpation.
Unicameral bone cysts are most commonly seen after pathologic fracture. On occasion, there will be swelling and tenderness.
Giant cell tumor of bone may cause swelling, pain, tenderness, and a sense of weakness. Loss of range of motion is common, as these lesions are typically periarticular. Pathologic fracture may be seen.
IMAGING AND OTHER DIAGNOSTIC STUDIES
Plain radiographs are indispensable in the initial evaluation of primary bone tumors (FIG 2A).
Magnetic resonance imaging (MRI) is useful when an aggressive lesion or soft tissue extension is suspected. MRI may allow better identification of the local extent of disease and may assist in operative planning (FIG 2B).
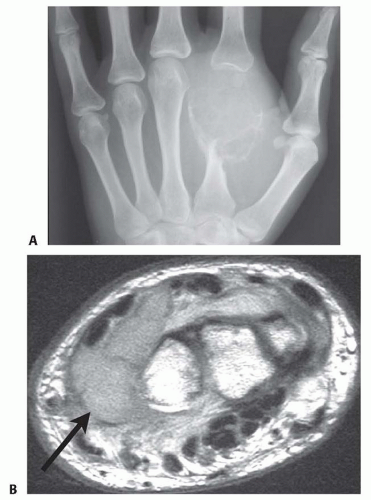
FIG 2 • A. Radiograph showing giant cell tumor of the metacarpal. B. MRI axial image of grade 3 giant cell tumor of the distal radius (arrow).
Grade 1 lesions are confined to the intramedullary cavity without distention or distortion of the cortex.
Grade 2 lesions distend the cortex but do not extend into the surrounding soft tissues.
Grade 3 lesions destroy the cortex and extend into the surrounding soft tissues.
Total body bone scan and lung computed tomography (CT) scan are required for staging patients with giant cell tumor of bone.
Incision or needle biopsy may be required when radiographs and MRI are not diagnostic.
DIFFERENTIAL DIAGNOSIS
Enchondroma
Chondromyxoid fibroma
Chondrosarcoma
Unicameral bone cyst
Infection
Aneurysmal bone cyst
Giant cell tumor of bone
Primary malignant bone neoplasms
Acrometastasis
NONOPERATIVE MANAGEMENT
Enchondromas and unicameral bone cysts may be observed provided radiographic assessment is diagnostic or the differential diagnoses are limited to benign, nonaggressive lesions with an indolent natural history. The assessment of risk of pathologic fracture is paramount. Lesions with a substantial risk of pathologic fracture in the context of the patient’s activity level are best treated operatively.
The rare risk of malignant degeneration of enchondromas should be considered and discussed with the patient.
Suspected giant cell tumor of bone requires biopsy. Rarely, these can be treated with radiation alone; however, this approach is the exception and should not be considered first-line treatment. Radiation is associated with a risk of subsequent true malignant degeneration to a highly malignant giant cell tumor of bone.
SURGICAL MANAGEMENT
All suspected giant cell tumors of bone and those enchondromas and unicameral bone cysts with a high risk of fracture are best treated surgically.
Preoperative Planning
The radiographic extent of disease must be assessed.
The approach will vary depending on the anatomic location.
Bone graft source (autologous or allograft) must be considered.
Precautions to prevent donor site cross-contamination must be considered and reviewed with the operating room team.
The surgeon must determine the anticipated need for frozen section and discuss this with the pathologist and review radiographs before any anticipated frozen section.
The surgeon must secure and confirm the availability of any necessary grafting materials, instruments, implants, or adjuvants (ie, liquid nitrogen).Related posts:
 Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations
Open Reduction and Internal Fixation of Displaced Lateral Condyle Fractures of the Humerus
Open Reduction and Internal Fixation of Capitellum and Capitellar-Trochlear Shear Fractures
Corrective Osteotomy for Radius and Ulna Diaphyseal Malunions
Volar Plating of Distal Radius Fractures
Ligament Stabilization of the Unstable Thumb Carpometacarpal Joint
Dorsal Block Pinning of Proximal Interphalangeal Joint Fracture-Dislocations

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


