Managing patients with peripheral nerve injuries (PNIs) in the trauma setting is particularly challenging. Concomitant central nervous system (CNS), orthopaedic, and vascular injuries easily confound the evaluation of limb function. Patients with PNIs also tend to have relatively high mean injury severity scores because of the frequent association with head injury, chest trauma, and spine fractures.1,2 During convalescence, the patient with PNI has a greater need of posthospitalization rehabilitative and social services than does the general trauma patient population.3
PNI is estimated to occur in 2% to 5% of multitrauma victims,4,5 often being diagnosed in a delayed manner after other more obvious and life-threatening issues have been addressed. Because diagnostic delay can mitigate functional outcomes and may sometimes bear medicolegal consequences, a rapid and reliable protocol for evaluating nerve injuries is important. Despite dramatic advances in soft tissue imaging and electrophysiologic evaluation, the most sensitive and cost-effective diagnostic tool remains a sound and thorough clinical examination. Current management practice for PNI is largely a derivative from experience gained in the treatment of large numbers of 20th century combat wounds.6 As in many areas of clinical practice currently, there is a dearth of class one evidence upon which to base our treatment decisions.
ANATOMY OF PERIPHERAL NERVES
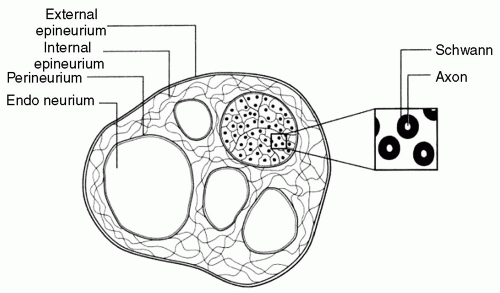
Peripheral nerves have three principal constituents: axons, the elongated cell processes of neurons which propagate nerve action potentials (NAPs); Schwann cells, which ensheathe axonal processes within a wrapper of myelin; and a connective tissue matrix, which itself has three components—the epineurium, the perineurium, and the endoneurium (see Fig. 1). The cell bodies of peripheral nerves reside in the ventral horn of the central gray matter of the spinal cord (motor fibers), in the dorsal root ganglia (sensory fibers), and in the paraspinal autonomic ganglia. Both neurotransmitters and structural cytoskeletal elements are manufactured within these neuronal cell bodies and are transferred centrifugally through processes of slow and rapid axoplasmic transport.
The three-layered connective tissue matrix organizes the fibers into small bundles termed fascicles. Schwann cells may envelope individual axons in a multilayered protective wrapping of myelin, as in the case of heavily myelinated “Ia fibers” that supply the muscle spindle, or a group of axons such as in unmyelinated “C fibers” responsible for pain sensation. The myelin investment acts as an electrical insulator promoting saltatory conduction jumping between the nodes of Ranvier, thereby considerably accelerating neural conduction velocity. Small unmyelinated pain fibers appear to be more susceptible to injury than are larger myelinated sensory or motor fibers.
Figure 1 Schematic cross-section of a peripheral nerve. (Grant GA, Goodkin R, Kliot M. Evaluation and surgical management of peripheral nerve problems. Neurosurgery. 1999;44:825-840.)
Proximally within a peripheral nerve there is an intermingling of motor, sensory, and autonomic fibers. Distally they segregate into separate fascicles grouped by function and target organ. This segregation is reflected in varying fascicular patterns: polyfascicular nerves have many differently sized fascicles; oligofascicular nerves have few fascicles; and monofascicular nerves consist of one large fascicle. As an example, the ulnar nerve is polyfascicular in the upper arm, transitioning to oligofascicular at the elbow, and terminating in monofascicular nerves in the fingers.7 The blood supply to peripheral nerves is relatively robust and is provided by longitudinally oriented vessels running within the epineurium. This permits telescopic lengthening and shortening of the vasculature associated with joint movement. Small collateral vessels branch obliquely from the parent trunk into the perineurium and endoneurium to give segmental supply to individual fascicles.8
CLASSIFICATION OF PERIPHERAL NERVE INJURY
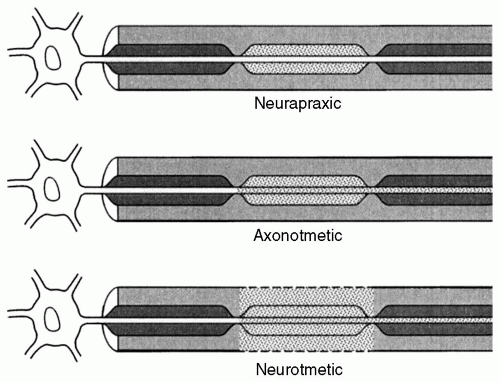
A clinically useful schema for classifying PNI is important for understanding mechanisms of injury and recovery, as well as for predicting clinical outcomes and guiding therapeutic interventions. Although quite simplistic, the well-known Seddon classification retains a high level of utility for these purposes (see Fig. 2).9 PNI is classified into three broad categories based on an idealized conception of the primary pathophysiology involved.
Figure 2 Schematic of Seddon classification of nerve injuries. (Grant GA, Goodkin R, Kliot M. Evaluation and surgical management of peripheral nerve problems. Neurosurgery. 1999;44: 825-840.)
Neuropraxic injury is the least severe form of injury. It is thought to arise from a transient conduction block resultant from a local perturbation of the ionic balances that sustain normal transmembrane electrical potentials. Because the nerve itself retains its physical integrity, the prognosis for spontaneous recovery is very good, although the myelin sheath can sometimes experience permanent damage. Recovery from neuropraxic injury is usually swift, with marked clinical improvement generally observed within hours to a few days.
Axonotmetic injury is more severe. The axon itself is disrupted with degeneration of the distal stump. However, the surrounding support structures including the endoneurial tubules and perineurial sheaths remain intact to a variable degree, leaving in place a conduit-guiding axonal outgrowth to appropriate reinnervation of target organs. The quality of recovery is dependent on the degree to which this intrinsic architecture has been maintained and the distance which the reparative axonal growth cone must traverse to its target (vide infra). Some cases may require surgical intervention if extensive scarring impedes axonal regeneration.
Neurotmetic injury is the most severe form of PNI and results in discontinuity of both the axon and the endoneurial conduits, either from internal scarring or by physical transection. This class of injury has the worst outlook for functional recovery despite optimal management, including surgical intervention.
Although the terminology of the Seddon classification continues to enjoy wide usage, the underlying pathophysiology in most cases of PNI is complex, incorporating several mechanisms of injury at variable locations in the nerve.10 The Sunderland classification expands the Seddon schema into five different grades of injury according to a more elaborate characterization of the imputed pathophysiolgy.11 (See Table 1.)
PATHOPHYSIOLOGY OF PERIPHERAL NERVE INJURY AND REGENERATION
Axonotmetic and neurotmetic injury unleash an inflammatory cascade leading to the distal degeneration of the nerve first described by Augustus Waller.12 Although all the mechanisms underlying Wallerian degeneration are not completely understood, a characteristic process of dissolution of the axoplasma and axolemma of the distal stump commences within 24 to 48 hours postinjury. Calcium ion influx and activation of axonal proteases are the initial signatures of this event. In the days and weeks subsequent to injury cytokine-activated macrophages continue this process.13
Recovery from PNI depends on the degree and type of injury. Neuropraxic injuries such as conduction blocks that are the result of a transient ischemic insult recover most rapidly. These are usually without significant structural disruption to the axon. Following axonotmetic injury, distal axonal sprouting can begin within the first several days. If endoneurial channels are preserved to guide axonal regeneration down preestablished pathways, regrowth can progress at a rate of 1 to 5 mm per day. Laceration injuries seem to recover more slowly than do crush injuries, even after surgical reapproximation.
TABLE 1 CLASSIFICATION SYSTEMS FOR PERIPHERAL NERVE INJURY
Seddon Classification
Sunderland Classification
Pathology
Prognosis
Neuropraxia
First degree
Myelin injury or ischemia
Excellent recovery in weeks to months
Axonotmesis
Axon loss Various stromal disruption
Good to poor depending on integrity of supporting structures and distance to muscle
Second degree
Axon loss Endoneurial tubes intact
Good depending on distance to muscle
Perineurium intact
Epineurium intact
Third degree
Axon loss
Poor
Endoneurial tubes disrupted
Axonal misdirection
Perineurium intact
Surgery may be required
Epineurium intact
Fourth degree
Axon loss
Poor
Endoneurial tubes disrupted
Axonal misdirection
Perineurium disrupted
Surgery usually required
Epineurium intact
Neurotmesis
Fifth degree
Axon loss
No spontaneous recovery
Endoneurial tubes severed
Surgery required
Perineurium severed
Prognosis after surgery guarded
Epineurium severed
(Adapted from Dillingham TR. Approach to trauma of peripheral nerves. In: 1998 AAEM Course C: Electrodiagnosis in traumatic conditions. Rochester: American Association of Electrodiagnostic Medicine; 1998:7-12; Robinson LR. Traumatic injury to peripheral nerves. Muscle Nerve. 2000;23:863-873.)
Much of this delay appears to occur at the site of the transection itself, where the advancing growth cone must bridge a physical gap and then find its way into existing endoneurial sheaths. In neurotmetic and the more severe grades of axonotmetic injury that are associated with endoneurial disruption, axonal regeneration can be slowed, misdirected, or even halted by intraneural scarring. This may ultimately result in neuroma formation. Recovery from demyelinating injuries is even slower and is dependent upon the location, degree, and the length of involvement.
Poor outcomes traditionally associated with more proximal PNI are believed to relate in part to the failure to achieve reinnervation in a timely manner. If target muscles are deprived of the trophic influences of neural input for more than 18 months, they become permanently damaged and are no longer receptive to reinnervation.14 Given that axonal regrowth proceeds at a rate of approximately 25 mm per month under optimal conditions, this essentially precludes successful reinnervation of muscles more than 40 to 45 cm remote from the site of axonotmetic injury or nerve repair. Besides the distance to target organ, other factors relevant for functional recovery include the degree of intraneural scarring, the proximity of severed nerve ends to one another, patient age, and the amount of misdirected reinnervation that occurs.15 The latter is especially problematic in proximal injuries to a peripheral nerve where there is extensive intermingling of the sensory and motor components and significant potential for misdirected reinnervation.
MECHANISMS OF INJURY
Common mechanisms of PNI include stretch, compression, ischemia, contusion, and laceration. Thermal, electrical, and injection injuries are less frequently encountered. In a civilian population, stretch and traction mechanisms account for approximately 70% of PNIs.16 These injuries occur once the nerve has been elongated beyond its elastic limit, imparting both a mechanical trauma and a microvascular insult. The classic case is that of a brachial plexus injury (BPI). According to the severity of the applied forces, injury may range from a very transient neuropraxic deficit to a permanent internal derangement affecting multiple elements of the plexus over an extended length.
The extreme form of this injury culminates in proximal avulsion of the constitutive rootlets of the plexus from the spinal cord itself. Peripheral nerves are also vulnerable to stretch where they travel in close proximity to a dislocated joint or a long bone fracture. Fractures of the midhumeral shaft causing a radial nerve injury are a well-known example of this phenomenon.17
Compressive injury is typified by the classic “Saturday night palsy.” In this case, the radial nerve is pinched against the underlying humerus by an external force. Although the nerve retains its physical continuity, a profound sensorimotor deficit can ensue. Combinations of mechanical deformation and microcirculatory arrest are implicated as causative factors. PNI is occasionally the result of an internally expanding hematoma (e.g., in the retroperitoneum affecting the lumbar plexus) or an expanding pseudoaneurysm (e.g., of the subclavian artery affecting the brachial plexus). Compartment syndromes in the forearm and calf are examples of injury by a primarily ischemic mechanism. The ischemic tolerance of various peripheral nerves is not fully known, but there is some evidence to indicate that vascular insufficiency in excess of 8 hours can lead to irreversible injury.18
The simplest form of penetrating injury is that of the sharp, clean laceration, as would be caused by a shard of glass or a knife wound. Missile wounds may be of low or high energy, and with or without fragmentation. High-energy and fragmentation wounds are associated with bony and ligamentous injury, as well as soft tissue loss. This mechanism is typical of a combat wound, the management of which is often further complicated by gross contamination. Blast effect and shock wave transmission in missile wounds may impart very damaging injury remote from the projectile trajectory, even where physical continuity of the nerve has been maintained. High-energy projectile wounds are often very difficult to repair for these reasons. Thermal and electrical PNIs are frequently associated with other significant soft injuries. Conservative treatment is usually advised, as aggressive management with extensive neural grafting has not improved outcomes for these patients.19
CLINICAL EVALUATION OF PERIPHERAL NERVE INJURIES
After identifying and stabilizing any life-threatening injuries, a thorough evaluation of peripheral nerve function should be included in the course of the secondary examination. A high index of suspicion should be adopted for patients with penetrating wounds in proximity to major nerve trunks (e.g., shoulder, volar forearm, buttock, groin, and popliteal fossa), and for those patients with certain joint dislocations and fractures known to be associated with PNI (see Table 2).
Examination should be systematic and standardized, beginning proximally and progressing distally. The existence of PNI is defined by motor and sensory deficits conforming to the anatomic distribution of named peripheral nerves. The limbs should be completely exposed and assessed for symmetry. Muscle tone and bulk and joint range of motion should be evaluated. Atrophy, fasciculation, and contractures all signify a prior injury unrelated to an acute trauma. Nor are spasticity, rigidity, or pathologic movements such as tremor features of PNI. Occasionally, a Tinel phenomenon can be provoked during the acute phase by lightly percussing over a partially injured nerve. This evokes characteristic electric paresthesias distally in the distribution of the affected nerve.
TABLE 2 FREQUENCY OF ORTHOPAEDIC INJURIES WITH ASSOCIATED PERIPHERAL NERVE INJURY
Inaba K, Sharkey PW, Stephen DJ, et al. The increasing incidence of severe pelvic injury in motor vehicle collisions. Injury, Int J Care Injured. 2004;35:759-765.
Functionally important muscle groups should be tested individually and throughout the range of motion of the associated joint. A detailed review of individual muscle testing is beyond the scope of this chapter, but the reader is referred to the excellent text, “Aids to the examination of the peripheral nervous system,”20 which includes pictorial demonstrations. Certain key index muscles and autonomous sensory zones can be quickly assessed to screen for a major PNI in patients whose condition precludes detailed examination (see Table 3).
For a workable and comprehensive motor assessment, we recommend the organizational method of Dr. Joseph Miller (personal communication): in the shoulder girdle, there are 7 readily testable muscles innervated by 6 peripheral nerves (see Table 4); there are 25 reliably testable muscles in the upper extremity, reflecting function in 5 major peripheral nerves (see Table 5); and in the lower limb, there are 19 testable muscles that demonstrate function in 8 peripheral nerves and their major branches (see Table 6). (Miller J, personal communication, 2003). The examiner should recognize that even alert and oriented patients might not put forth a full effort in the presence of pain or for reasons of secondary gain.21 The examiner should also be aware that certain adaptive movements undertaken to compensate for functional deficits could sometimes mask weakness. A common example of this is the substitution of the brachioradialis muscle for the biceps brachii to accomplish elbow flexion while holding the forearm halfway between pronation and supination. Palpation of the muscle belly during motor testing helps clarify these situations.
TABLE 3 QUICK EVALUATION OF MOTOR AND SENSORY FUNCTION BY NERVE
A full sensory evaluation includes testing of light touch, pinprick sensitivity, vibration, proprioception, two-point discrimination, stereognosis, and graphesthesia. In the acute setting, the circumstances of examination and the patient’s own level of consciousness may preclude such exhaustive testing. Light touch and pinprick testing are usually the most informative. Both dermatomal and cutaneous sensory distributions for peripheral nerves are relatively consistent (see Fig. 3).22 Recognizing the pattern of sensory loss can be extremely helpful in distinguishing a PNI from a radicular (dermatomal) or spinal cord (segmental) injury. However, there is sufficient variability and overlap in the distribution of peripheral nerves to sometimes obscure a clear-cut sensory deficit to correspond with motor findings in some cases of PNI. Additionally, as many nerve injuries are incomplete, different modalities may be differentially affected. It is not uncommon for a patient to experience loss of nocioception or two-point discrimination, while maintaining a relatively acute sense of light touch. Despite the inconsistencies and incongruities that sometimes emerge during sensory testing, documentation of the patient’s baseline examination and the quality of that examination are important. It will facilitate accurate diagnosis of neurologic injury, enable trending of function, and occasionally has medicolegal relevance.
TABLE 4 SHOULDER GIRDLE
Nerve
Group
Muscle
Spinal accessory
Back
Trapezius
Long thoracic
Serratus anterior
Thoracodorsal
Latissimus dorsi
Dorsal scapular
Scapular
Rhomboid
Suprascapular
Supraspinatus
Suprascapular
Infraspinatus
Pectoral (medium and lateral)
Odd
Anterior pectoralis
TABLE 5 UPPER EXTREMITY PERIPHERAL NERVES AND MUSCLES TO BE TESTED
Nerve
Group
Muscle
Axillary
Deltoid
Musculocutaneous
Biceps
Radial (extensor)
Odd
Triceps
Brachioradialis
Supinator
Forearm
Extensor carpi radialis longus
Extensor carpi ulnaris
Extensor digitorum
Thumb
Extensor pollicis longus
Extensor pollicis brevis
Abductor pollicis longus
Median (flexor)
Odd
Pronator Teres
Forearm
Flexor carpi radialis
Flexor digitorum sublimes
Flexor digitorum profundus I/II
Thumb
Flexor pollicis longus
Opponens pollicis
Abductor pollicis brevis
Ulnar (hand)
Odd
Flexor carpi ulnaris
Little finger
Abductor digiti minimi
Opponens digiti minimi
Flexor digitorum profundus III/IV
Thumb
First dorsal interosseous
First volar interosseous
Adductor pollicis
The most commonly accepted methods of grading strength and sensation are based on the well-known British Medical Research Council (BMRC) 1 to 5 scales (see Tables 7 and 8).23 Although widely employed, the BMRC motor scale is deficient in its quantification of the frequently encountered condition of a muscle that is weak, but stronger than antigravity (grade 4). The Louisiana State University Medical Center (LSUMC) grading scale attempts to address this deficiency with a more precise and reproducible characterization of sensorimotor function24 (see Tables 9 and 10). As we become more sophisticated in our management of PNI, the LSUMC scale will probably find wider currency.
Only gold members can continue reading. Log In or Register to continue