TBI is a serious public health problem in the United States. Each year, an estimated 1.7 million people sustain a TBI.1 Of them
52,000 die,
275,000 are hospitalized, and
1.365 million, nearly 80%, are treated and released from an emergency department.
TBI is responsible for a third (30.5%) of all injury-related deaths in the United States.1
TBI is more common in children aged 0 to 4 years, adolescents aged 15 to 19 years, and adults aged 65 years and older. Adults aged 75 years and older have the highest rates of TBI-related hospitalization and death. TBI rates are higher for males than for females.
Blasts are a leading cause of TBI for military personnel in war zones.2
Direct medical costs and indirect costs such as lost productivity because of TBI totaled an estimated $60 billion in the United States in 2000.3
Primary injury occurs at the time of impact and results from the shear forces of the impact (Fig. 22-1).
Secondary injury follows primary injury and is the effect of cerebral and extracerebral insults. It occurs at both a macroscopic level and a cellular level.
The mechanisms of secondary injury are classified under four categories4 (Table 22-1):
Ischemia, excitotoxicity, energy failure, and cell death
Cerebral swelling
Axonal injury
Inflammation and regeneration
Theories of Recovery: At least three different theories have been proposed to explain the recovery that follows a brain injury and include a reversal of diaschisis, compensation, and adaptive plasticity. Diaschisis is a temporary reduction in function of structures interconnected with an injured brain. Functional recovery is likely to be related to a gradual reduction in diaschisis.
Compensation is the use of alternative strategies as an individual attempts to supplement lost function.
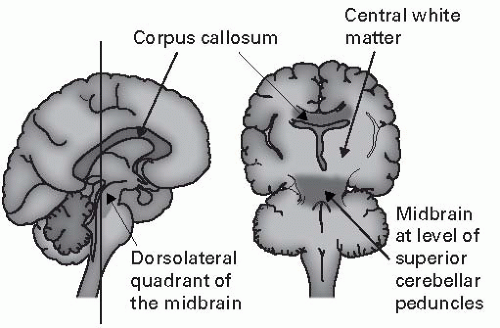
Figure 22-1 Brain regions particularly involved in diffuse axonal injury include the corpus callosum and parasagittal white matter as well as the dorsolateral quadrants of the midbrain.
Adapted from Auergach SH. Neuroanatomical correlates of attention and memory disorders in traumatic brain injury: an application of behavioral subtypes. J Head Trauma Rehabil. 1986;1:1-12.
A third theory is that functional recovery is largely dependent upon neuroplasticity of intact remaining brain structure. Underlying mechanisms include unmasking of existing connections, long-term potentiation, long-term depression, axonal sprouting, dendritic sprouting, synaptogenesis, and angiogenesis (Table 22-2).5
Glasgow Outcome Scale: The Glasgow Outcome Scale (GOS) is a five-level score:
Dead
Vegetative state
Severely disabled
Moderately disabled
Good recovery
Posttraumatic Amnesia (PTA): the duration during which patients neither encode nor retain any new information and experience and can be assessed by Galveston Orientation Amnesia Test (GOAT). The end of PTA is marked by a score of >75 on GOAT on two consecutive days (Table 22-3).
In the future, a combination of clinical, laboratory (serum biomarkers and genetic markers), evoked potentials, and radiological techniques (functional MRI and MR spectroscopy) may need to be used for prognostication (Table 22-4).
TABLE 22-1 Comparison of Clinical Features Associated with Coma, Vegetative State, Minimally Conscious State, and Locked-In Syndrome
Condition
Consciousness
Sleep/wake
Motor function
Auditory function
Visual function
Communication
Emotion
Coma
None
Absent
Reflex and postural responses only
None
None
None
None
Vegetative state
None
Present
Postures or withdraws to noxious stimuli
Occasional nonpurposeful movement
Startle
Briefly orients to sound
Startle
Brief visual fixation
None
None
Reflexive crying or smiling
Minimally conscious state
Partial
Present
Localizes noxious stimuli
Reaches for objects
Holds or touches objects in a manner that accommodates size and shape
Automatic movements (e.g., scratching)
Localizes sound location
Inconsistent command following
Sustained visual fixation
Sustained visual pursuit
Contingent vocalization
Inconsistent but intelligible verbalization or gesture
Contingent smiling or crying
Adapted from Disorders of Consciousness: Giacino JT, Ashwal S, Childs N, et al. The minimally conscious state: definition and diagnostic criteria. J Neurol. 2002;58:349-353, Special Article.
Only gold members can continue reading. Log In or Register to continue