Trauma is the leading cause of death for both pregnant and nonpregnant woman in their childbearing years.1 Approximately 5% of all pregnancies are complicated by trauma.2,3,4 Of woman aged between 12 and 51 who are listed in the National Trauma Databank, 1.5% were injured while pregnant. The rate of mortality for the pregnant mother is 1.4% and the rate of fetal demise in pregnant woman following traumatic injury is 6.1%.4 The preponderance of trauma during pregnancy is due to a blunt mechanism of injury with penetrating trauma being relatively infrequent. Motor vehicle accidents account for more than 50% of all traumas during pregnancy and most fetal deaths (82%) from trauma are due to motor vehicle accidents.5,6 The pregnant female is at risk for trauma from the following etiologies in descending order: motor vehicle accidents, domestic abuse and assault, falls, and burns.5 Domestic assault is an important and often overlooked cause of trauma in pregnant patients.
Central to the management of traumatic injury of the pregnant patient is the fact that two separate, but linked patients are involved. A key principle is to treat the mother first because most medical measures which aid in the resuscitation of the mother will be helpful to the fetus. Assessment and patient management can be complicated by the anatomic and physiologic changes of pregnancy. These changes can mimic or camouflage injury and result in a patient who can be difficult to characterize. A multidisciplinary approach to the patient that includes specialists from trauma surgery, emergency medicine, obstetrics, nursing, and prehospital providers is strongly recommended. Ultimately, trauma management of the pregnant patient revolves around minimizing fetal loss and optimizing both the maternal and fetal outcome.
PHYSIOLOGY
Many changes occur to the anatomy and physiology of a pregnant woman throughout the gestational period. These changes influence the pattern of injury, assessment, and management of the pregnant trauma patient. A summary of these changes is provided in Table 1.
Reproductive Organs
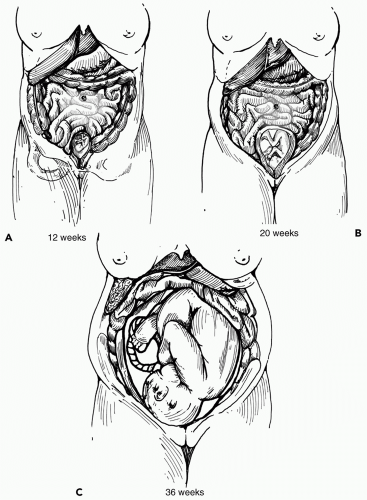
The most obvious physical change during pregnancy is the gradual enlargement of the uterus (see Fig. 1). At 12 weeks’ gestation, the uterus transitions from being a pelvic organ to becoming an intraabdominal organ by rising over the pelvic brim.7 Around 20 weeks’ gestation, the vertex of the gravid uterus can be palpated at the level of the umbilicus. At 36 weeks of gestation, the uterus has reached the costal margins and in the last few weeks of pregnancy the fundal height decreases as the fetal head drops back into the pelvis. Concomitant with uterine enlargement is the displacement of maternal abdominal organs laterally and cephalad. In the late stages of pregnancy, most of the gastrointestinal tract is located above the inferior costal margin. The diaphragm may be elevated with corresponding compression of the lungs and mediastinum. Uterine blood flow increases from 50 mL per minute at 10 weeks’ gestation to 500 mL per minute in the term female, which is equivalent to 17% of the cardiac output.8 Compensatory dilation of the uterine and pelvic veins will occur to handle this increased blood flow. This increase in vascularity can result in massive hemorrhage with pelvic injury.
Cardiovascular
By the end of the first trimester, the plasma volume increases by 40% to 50% and a smaller increase in red cell volume is also present (20% to 30%).9 The result is the physiologic anemia of pregnancy and in late pregnancy a hematocrit of 31% to 34% is normal.7 This hypervolemia is meant to compensate for the 1 to 1.5 L hemorrhage that occurs at childbirth. The pregnant patient also experiences a decrease in peripheral vascular resistance resulting in supine hypotension, a decrease in blood pressure of 15% to 20%, and an increase in cardiac output by up to 40%. These changes nadir at 28 weeks’ gestation and can mask signs of acute blood loss.10,11,12 Gravid patients can experience traumatic hemorrhage of up to 2,000 mL without demonstrating clinical deterioration through the typical signs and symptoms of shock.
TABLE 1 PHYSIOLOGIC CHANGES DURING PREGNANCY
Organ System
Normal
Pregnant
Reproductive organs
Uterine location
Pelvis
Abdomen
Uterine blood flow (mL/min)
50
500-700
Cardiovascular
Cardiac output (L/min)
5-6
↑ 30 %-40%
Heart rate (beats/min)
70-80
↑ 15-20 beats/min
Blood pressure (mm Hg)
110/70
↓ 10-15 mm Hg second trimester, normal at term
Respiratory
Tidal volume (mL)
450
↑ 30%-50%
Respiratory rate (breaths/min)
12-16
↑ 15%
Functional residual capacity (mL)
1,800
↓ 25%
Oxygen consumption (mL/min)
250
↑ 20%
pH
7.34-7.44
7.41-7.46
Pao2 (mm Hg)
95-100
↑ 105
Paco2 (mm Hg)
35-45
↓ 27-32
Hco3 (mmol/L)
24-30
↓ 19-24
Diaphragm
Normal
Elevated up to 4 cm
Gastrointestinal
Lower esophageal sphincter
Normal
Relaxed, predisposes to GERD and aspiration
Hepatobiliary
Normal
↑ Progesterone results in ↓ cholecystokinin, cholestasis and ↑ gallstone formation
The amount of replacement fluid needed in a pregnant patient changes as the plasma volume increases. A third trimester patient can require 1.5 times the amount of intravenous fluid resuscitation to compensate for the same level of hemodynamic compromise in a nonpregnant patient.13 The gravid uterus can lead to supine hypotension by direct compression of the inferior vena cava that diminishes venous return. This can be minimized by using a foam wedge or rolled blanket to displace the backboarded patient to a moderate left-lateral decubitus position during transport and resuscitation. This maneuver should be employed to improve blood flow in patients >20 weeks’ gestation.
Respiratory
Progressive uterine enlargement results in elevation of the diaphragm as abdominal organs are displaced. A rise in the resting level of the diaphragm by as much as 4 cm occurs.14 This results in a decreased residual volume, an increase in the diaphragmatic excursion, and results in larger tidal volumes. At 12 weeks of gestation, the functional reserve capacity decreases by 10% to 25%.13 Consequently, apnea is poorly tolerated and supplemental oxygen should always be given to pregnant trauma patients. Mild hyperventilation leads to respiratory alkalosis and a shift in the oxyhemoglobin dissociation curve to the left, increasing the maternal affinity for hemoglobin to be bound to oxygen. A increase in the pH level leads to a simultaneous rise in the level of 2,3 diphosphoglycerate, which shifts the oxyhemoglobin dissociation curve back to the right and facilitates the unloading of oxygen from maternal hemoglobin to fetal hemoglobin across the placenta.15,16
Figure 1 A-C: Enlargement of the uterus and fundal height during pregnancy.
Gastrointestinal
Progressive enlargement of the uterus stretches out the abdominal wall and displaces the abdominal viscera. The response to peritoneal irritation is altered and the change in organ location can make the physical examination confusing and potentially unreliable. Compression of the gastrointestinal viscera cephalad, diminished motility, and hormone-mediated relaxation of the lower esophageal sphincter can predispose the gravid patient to gastroesophageal reflux disease and increase the risk of aspiration.17 A high level of the female hormone progesterone inhibits cholecystokinin production resulting in decreased gallbladder contractility. This leads to cholestasis and an increase in the susceptibility to gallstone development.18
Hematologic
Pregnancy increases the cellular synthesis of many procoagulant factors; however, most pregnant women have normal anticoagulant factor levels except for a decrease in protein S.19 In total, pregnancy is a hypercoagulable state but bleeding time and clotting time are unchanged when measured. The risk of deep venous thrombosis and venous thromboembolism is markedly increased in pregnancy.20 Platelets are more reactive and their destruction is enhanced. Most pregnant patients have an increased production of platelets within the bone marrow. The relative leukocytosis of pregnancy is well known and accounts for a slight rise in the overall white blood cell count. Blood volume increases and total red blood cell mass may be 30% higher in the pregnant patient despite a drop in the measured circulating hemoglobin per unit volume.
Musculoskeletal
Interosseus ligaments soften and relax during pregnancy. This results in increased mobility and laxity of joints such as the sacroiliac, and symphysis pubis in preparation for expansion of the birth canal. These changes in addition to uterine enlargement affect the pregnant female center of gravity and gait such that they are predisposed to falls.
PREGNANT PATIENT ASSESSMENT AND MANAGEMENT
Prehospital
The initial care of the patient is usually by prehospital personnel at the scene and in transport. To begin resuscitation and treatment of the patient, it is essential that prehospital providers be aware of the physiologic changes present in the pregnant patient. Provision of the Airway, Breathing, and Circulation (ABCs) of trauma care is paramount to both the mother and fetus. Awareness of airway management problems such as tissue edema in the oropharynx is essential. The relative hypervolemia of pregnancy may mask the signs and symptoms of blood loss and shock until an acute rapid decompensation occurs. Intravenous solutions should be administered in a liberal manner during transport to avoid sudden deterioration in a compensated, but injured patient. These patients should be transported with spine precautions on a backboard tilted to the left to avoid uterine compression of the vena cava.21 In addition to the standard patient history, appropriate information regarding prenatal care, gestational age, and pregnancy complications should be obtained and relayed to the accepting trauma center when feasible.
Primary Survey
The conduct of the primary survey in the pregnant patient is the same as for the nonpregnant patient. The goal is to identify, triage, and treat life-threatening injuries by addressing ABC with the mother given treatment priority. Assessment and establishment of the maternal airway is critical and all pregnant patients should receive supplemental oxygen at a minimum. Late in gestation the oropharynx is swollen from tissue edema and endotracheal intubation of the gravid patient can be difficult; therefore, use of a smaller than normal diameter endotracheal tube, such as a 6.5 mm ID or less, may be necessary.22 Injury can stimulate a stress response release of catecholamines. Maternal catecholamine surges can lead to uterine-placental vasoconstriction that can compromise the delivery of oxygen to the fetal circulation.23 Small differences in the maternal Pao2 can markedly change the oxygen saturation of the fetal blood because of a leftward shift in the fetal oxyhemoglobin dissociation curve when compared to the maternal curve.24 Aggressive crystalloid intravenous fluid resuscitation is recommended in the pregnant patient, even if evidence of hemodynamic compromise is not immediately apparent. Late in pregnancy, supine hypotension is present due to vena cava compression. This should be alleviated by placing the patient in a mild left lateral decubitus position using a wedge or rolled blankets placed under the transport backboard.
Secondary Survey
After the ABCs of the primary survey have been addressed, the secondary survey is performed. A brief, focused history should be obtained if the patient is not obtunded. Areas of importance include circumstances of the traumatic event, loss of consciousness, medical and obstetric history, time of last meal, medications, allergies, and a review of systems. A head-to-toe physical examination is carried out including a pelvic examination. Radiologic studies appropriate to the trauma evaluation should be ordered and usually include a chest and pelvic x-ray for the blunt trauma patient. A Foley catheter should be placed to monitor urine output and consideration should be given to placing a nasogastric tube given the pregnant patient’s likelihood of vomiting and risk for aspiration. Fetal monitoring is initiated during the secondary survey.
Obstetric history includes date of last menstrual period, expected delivery date, status of the current pregnancy, history of fetal movement, history of pregnancy-related medical problems such as gestational diabetes, preeclampsia, congenital disorders, preterm labor, placental abruption, placental previa, and prior fetal outcomes. Gestational age can be estimated using fundal height measured by palpation on the physical examination. Fundal height at the umbilicus is consistent with 20 weeks fetal gestation.24 Fetal viability is considered feasible approximately 24 to 26 weeks gestation, but can vary depending on the experience of the local neonatology support.25 A pelvic and rectal examination should be performed by an experienced team member, and attention must be focused on evidence of vaginal discharge (blood or amniotic fluid), cervical effacement and dilation, fetal station, and umbilical cord prolapse. Obstetrical presence as part of the trauma team effort in the evaluation of the gravid patient is highly recommended.
Five conditions are associated with signaling an acute status of the pregnancy. These include vaginal bleeding, rupture of amniotic sac, presence of contractions, bulging perineum, and abnormal fetal heart rate and rhythm.24 Vaginal bleeding before the onset of full-term labor is abnormal. It is potentially indicative of preterm labor, placental abruption, or placenta previa. Rupture of the amniotic sac can allow prolapse of the umbilical cord resulting in compression of the cord and potential compromise of the fetal circulation. Suspected amniotic fluid can be tested using Nitrazine paper, which will turn deep blue if the test is positive. Rupture of the amniotic sac is an obstetrical emergency because of the risk of infection and umbilical cord prolapse. Bulging of the perineum represents pressure from a presenting part of the fetus and delivery or spontaneous abortion may be in progress. The presence of strong contractions ascertained on the physical examination is associated with true labor and preparations should be made for delivery and resuscitation of the neonate.
Only gold members can continue reading. Log In or Register to continue