Introduction
Of all the patients presenting with carpal injuries, 10% have isolated carpal fractures. Of these injuries, around two-thirds affect the scaphoid; the other bones are involved less frequently in the order triquetrum (15%), trapezium (6%), pisiform (4%), capitate (2%), hamate (2%), lunate (1%), and trapezoid (<1%). Although this distribution is still controversial and details vary from one published series to another (see ▶ Table 5.1).
In common with scaphoid fractures, other carpal bone injuries that occur mainly in young men are underdiagnosed, and have a significant rate of complications. A high level of clinical suspicion is needed for their diagnosis. Taking an accurate history of the injury, carrying out a clinical examination looking for the area of tenderness, and obtaining appropriate sectional images (often by computed tomography [CT]) are required for making a decision on optimum management.
5.2 Fractures of the Trapezium
Fractures of the trapezium are often associated with other fractures, mainly of the thumb metacarpal and the distal radius. The commonest mechanism of injury is a shearing force applied to the first web space by an object held in the hand, for example the handlebar of a motorbike involved in a collision. Depending on the angle at which the force is exerted, a fracture of the base of the metacarpal or of the trapezium, or of both, will occur.
Five different patterns of fracture have been described:1 (a) vertical transarticular fracture, (b) horizontal fracture, (c) fracture of the dorsoradial tuberosity, (d) fracture of the anteromedial ridge, and (e) comminuted fracture. The commonest pattern is the vertical transarticular fracture (▶ Fig. 5.1). Radiographs of the thumb and the wrist are required in order to exclude other fractures. If undisplaced, conservative treatment in a cast for 4 to 6 weeks is indicated. If there is significant displacement, then reduction and stabilization are advised.

Fig. 5.1 (a and b) Vertical fracture of the trapezium in a teenager. Note the buckle fracture at the base of the thumb metacarpal. This fracture was treated with open reduction and internal fixation with two screws.
Comminuted fractures of the trapezium have been treated by external fixation, with acceptable results. These are often not a good indication for internal fixation, particularly if there is gross comminution. The alternative is to proceed to a primary trapeziectomy and suspensionplasty if the injury is an isolated fracture of the trapezium. However, this should not be done if there are other carpal fractures, because there is a risk of causing instability.
The ridge of the trapezium is the palmar projection of the bone on the medial corner, where the transverse carpal ligament is inserted. Fractures of the ridge are usually a consequence of a fall on an outstretched hand. In a direct mechanism the radial side of the wrist hits the floor. In an indirect mechanism the wrist comes into contact with the floor, causing a splaying of the carpal arch and producing an avulsion fracture of the insertion of the transverse carpal ligament from the trapezium, or from the hook of the hamate, or both. These fractures are probably underdiagnosed. Patients present with symptoms of pain and tenderness over the base of the thenar eminence and with thenar pain upon resisting wrist flexion. The author retrospectively reviewed 100 CT scans of the wrist, ordered for a suspected scaphoid fracture, and in 6 cases there was a fracture of the ridge of the trapezium (▶ Fig. 5.2). None of them were reported by the clinicians involved.
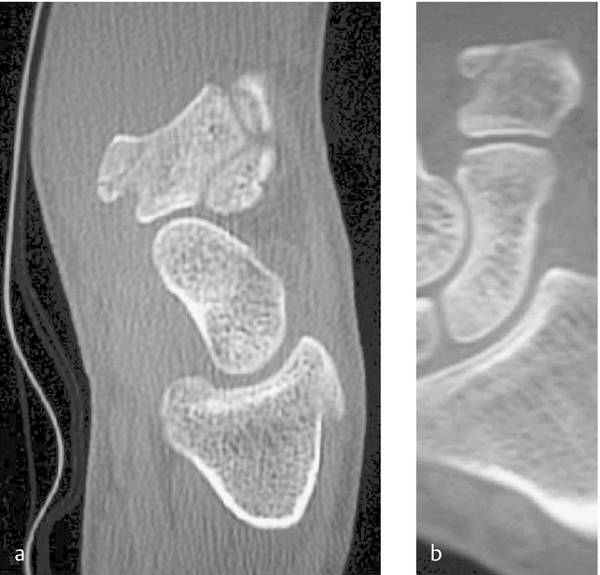
Fig. 5.2 (a and b) This patient presented with pain on the palmar—radial aspect of his wrist after a fall on outstretched hand. A scaphoid fracture was suspected but radiographs did not show an injury. CT scan shows a fracture of the ridge of the trapezium.
There are two types of fracture of the ridge of the trapezium: type I through the base of the ridge, and type II avulsions of the tip of the ridge.2 If a fracture is suspected, a CT scan will show the injury and show whether or not there is displacement. Undisplaced fractures heal well if immobilized. Displaced fractures may result in nonunion; if they remain painful, surgical excision of the fragment is recommended.
5.3 Fractures of the Capitate
Fractures of the capitate can be part of a greater arch perilunate injury or a consequence of a crush injury to the wrist with multiple bones involved. Isolated fractures of the capitate are infrequent, representing 2% of carpal fractures. Four patterns of fracture have been described: (a) transverse fracture of the proximal pole, (b) transverse fracture of the body, (c) vertical fracture in the coronal plane, and (d) sagittal plane fracture.3
Fenton described the fracture of the scaphoid and the proximal pole of the capitate4 and the mechanism was studied by Stein and Siegel5 (▶ Fig. 5.3). Unfortunately, these fractures are still often missed, resulting in long-term pain and loss of movement (▶ Fig. 5.4
Related posts:
 Undisplaced Scaphoid Fractures
Undisplaced Scaphoid Fractures
 Proximal Row Fractures (Other Than Scaphoid and Pisiform Fractures): Triquetrum and Lunate Fractures
Proximal Row Fractures (Other Than Scaphoid and Pisiform Fractures): Triquetrum and Lunate Fractures
 Role of Hand Therapy in the Treatment of Distal Radius Fractures
Role of Hand Therapy in the Treatment of Distal Radius Fractures
 Intra-articular Fractures of the Distal Radius (AO type C3), (Dry) Arthroscopic Approach
Intra-articular Fractures of the Distal Radius (AO type C3), (Dry) Arthroscopic Approach
 Galeazzi Fracture-dislocation
Galeazzi Fracture-dislocation
 Unstable Ulnar Styloid Fracture
Unstable Ulnar Styloid Fracture
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


