Abstract
Objective
To translate into Arabic and validate the “American Shoulder and Elbow Surgeons Evaluation Form” (ASES) for use in a Tunisian population presenting with periarticular pathologies of the shoulder.
Background
No functional index assessing the functional capacities of the shoulder is presently available in Arabic.
Patients and methods
The translation was achieved by means of forward/backward translation. Adaptations were carried out subsequent to a preliminary test involving 15 persons. Patients with periarticular shoulder disabilities were included. Clinical measurements evaluated pain and functional disability by means of the visual analogue scale (VAS). Interrater concordance (repeatability) was assessed using the intraclass correlation coefficient (ICC) and the Bland and Altman method. Construct validity (convergent and discriminant validity) was investigated using the Spearman rank correlation coefficient and a factorial analysis followed by orthogonal rotation. The internal consistency of each factor was graded in terms of the Cronbach alpha coefficient.
Results
Eighty (80) patients were included in the study. Interrater concordance was excellent (ICC = 0.96). The Bland and Altman method showed a low-variability mean difference. Correlations of the index score with the pain VAS ( r = −0.49) and functional disability ( r = −0.58) suggested satisfactory convergent validity, and our index likewise showed good discriminant validity. Factorial analysis led to the extraction of two factors with a cumulative variance rate of 92.6% that could not be explained.
Conclusion
Translated into Arabic, the ASES index was found to possess high metrological qualities. While the index has been satisfactorily validated with regard to a Tunisian population, additional studies are needed to verify its applicability to other Arab populations.
Résumé
Objectifs
Traduction en arabe et validation de « l’American Shoulder and Elbow Surgeons Evaluation Form » (ASES) sur une population tunisienne ayant des pathologies périarticulaires de l’épaule. Aucun indice fonctionnel n’est actuellement disponible en langue arabe pour évaluer les capacités fonctionnelles de l’épaule.
Patients et méthodes
La traduction a été obtenue par la méthode de « translation/back-translation ». Des adaptations ont été apportées après un prétest effectué sur 15 personnes. Ont été inclus dans cette étude les patients ayant des pathologies périarticulaires de l’épaule. Les mesures cliniques comprenaient surtout l’évaluation de la douleur et de l’incapacité fonctionnelle par l’échelle visuelle analogique (EVA). La reproductibilité a été évaluée par le coefficient de corrélation intraclasse (CCI) et la méthode de Bland et Altman ; la validité de construit (validités de convergence et de divergence) a été évaluée à l’aide du coefficient de corrélation de Spearman et d’une analyse factorielle suivie de rotation orthogonale. La cohérence interne de chacun des facteurs a été jugée par l’étude du coefficient alpha de Crohnbach.
Résultats
Quatre-vingts sujets ont participé à cette étude. La reproductibilité est excellente (ICC = 0,96). La méthode de Bland et Altman montre une moyenne des différences centrée. Les corrélations du score de l’indice avec l’EVA douleur ( r = −0,49) et incapacité fonctionnelle ( r = −0,58) suggèrent une validité de convergence satisfaisante. Notre indice avait de même une bonne validité de divergence. L’analyse factorielle a permis d’extraire deux facteurs avec un taux de variance cumulée de 92,6 % mais qui n’ont pas pu être expliqués.
Conclusion
L’indice ASES traduit en arabe a des qualités métrologiques satisfaisantes. L’indice est validé sur une population tunisienne, d’autres études sont nécessaires pour vérifier son applicabilité sur d’autres populations arabes.
1
English version
1.1
Introduction
Functional outcome may be highly important in shoulder pathology, as it affects not only professional capacities, but also activities in daily life. While the clinical examination is also important in assessment of shoulder pathology, it does not indicate the repercussions of the ailment on the patient’s daily routine. Conversely, functional assessment takes on a primordial role in shoulder pathology, since one of the essential goals in any treatment of this pathology is to improve functioning .
Several tests and indexes have been drawn up in order to evaluate functioning of the upper limb; while some of them specifically address shoulder instability or disability, others are used with regard to pathologies of which the scope includes the upper extremities.
One of these indexes is the Disabilities of the Arm, Shoulder and Hand scale (DASH), which is a self-administered and region-specific questionnaire that is not focused on any single pathology . It consists in 30 different items divided into four fields: symptoms, physical function, social function, psychological function. In its original English-language version, the DASH scale possesses high metrological qualities. Up until now, it has been translated and adapted in French, in Chinese, in German, in Greek, in Japanese, in Korean, in Spanish, in Russian, in Norwegian, in Swedish and in Turkish . There now exists a short version of the DASH (quickDASH) covering 11 of the 30 items in the full-length DASH; it has been validated in the original language and shown satisfactory metrological qualities. Indeed, the measurements obtained by quickDASH are sufficiently reliable to allow it to be used instead of the DASH scale, in evaluation of upper extremity pathologies .
The Shoulder Pain Disability Index (SPADI) is a self-administered questionnaire focused on the shoulder and consisting in 13 items evaluating physical and social aspects; five items involve pain, and eight items pertain to disability . It possesses good metrological qualities, and is one of the most widely used indexes in clinical studies.
Another specific index that may be cited is the “American Shoulder and Elbow Surgeons Evaluation Form” (ASES), which is widely used in functional assessment of shoulder pathologies ( Appendix A ). It is often used in postoperative evaluation of pathologies involving the rotator cuff, unstable shoulders, and the acromioclavicular (AC) joint .
The objective of our study was to translate into Arabic the ASES and to consider its metrological value in a Tunisian population.
1.2
Materials and methods
1.2.1
The index
The ASES is a self-administered questionnaire consisting in ten items. These items correspond respectively to the abilities to throw a ball with one hand, to sleep comfortably on the painful or affected shoulder, to get dressed unassisted, to wash one’s back, to manage toileting, to wash one’s hair alone, to lift 10 pounds above the shoulder, to reach a high shelf, to do routine tasks throughout the day, and to practice a usual sport or hobby.
Each item is accompanied by four levels of answers ranked from 0 to 3: answer 0 corresponds to total inability to perform the task; answer 1 corresponds to ability to perform the task with moderate trouble; answer 2 corresponds to ability to perform the task with slight trouble; answer 3 corresponds to ability to perform the task with no trouble.
Interpretation of the overall score involves addition of the figures given in the answers to the ten questions and allows for a total score ranging from 30 (no functional trouble) to 0 (maximum trouble). Cross-multiplication: total score (TS) divided by 0.3 (TS/0.3) places the score on a scale ranging from 0 to 100, which may be interpreted more intuitively: 100 (no functional trouble) to 0 (maximum trouble) .
Translation into Arabic was carried out in accordance with the forward/backward method and independently performed by three bilingual translators. The translations were then submitted for criticism to three experts (two doctors in physical medicine and one professional translator) to test their intelligibility and to provide the adaptations necessary from a linguistic as well as a cultural standpoint. A synthesis of the different translations yielded a definitive Arabic version that was at once quite close to the original version, and written in a literarily simple langue that even illiterates would easily understand.
A backward translation from Arabic into English was then performed by two other professional translators who had not been informed about the desired characteristics of their instrument; the backward translations were subsequently compared and contrasted with the original version.
1.2.2
Adapting the questionnaire
When a given concept has no equivalent in Tunisian culture, it was decided to totally modify the particular item so as to adapt it to the cultural context. The final version was then reviewed by the committee of experts in order to bring about the necessary adaptations. During this step, not only linguistic differences but also difficulties in translation, cultural diversity and conceptual equivalences became evident.
1.2.3
Preliminary test
The translated scale was tested on a group of 15 persons taken from the general population (pretest) in order to verify the acceptability of the questionnaire through evaluation of how the questions were understood and the number of missing answers. By the end of this step, an intermediate scale had been constructed.
1.2.4
Study of the series
1.2.4.1
Patients
Our study included patients aged from 20 to 80 years presenting with one of the following extra-articular pathologies of the shoulder: tenopathy, rupture of the rotator cuff or frozen shoulder syndrome. Diagnosis was based on a focused clinical examination of the shoulder completed by ultrasound in the event of a suspected rotator cuff injury. The study excluded all patients presenting with acute pathological states, inflammatory or infectious shoulder arthritis, a tumor-associated or bone-related pathology of the shoulder, a pathology of the elbow, wrist or hand, a paralyzed shoulder, serious psychiatric disorders or mental debility and refusal to participate in the study. Clinical and demographic data were collected for all the patients.
1.2.4.2
Methods
The questions were enunciated word by word, as they had been written. While the investigator could not modify the words, he was allowed to repeat the questions. Incomprehensible questions were eliminated. Statistical analysis of the answers was then carried out in order to select the questions for the final scales. With regard to each item, response distribution was analyzed; in cases where the distribution was not good (ceiling effect or floor effect), the item was eliminated.
The intraclass correlation coefficient (ICC) was used with regard to the interrater concordance for each item; when a question’s ICC was lower than 0.7, it was eliminated.
By the end of this step, a final version had been achieved.
1.2.5
An assessment of the metrological properties of the final version
1.2.5.1
Feasibility and acceptability
The relative feasibility and acceptability of the scales were appraised in terms of the number of missing data for each item, of how the questions put forward were understood, and of the time needed to complete the questionnaire.
1.2.5.2
Interrater concordance
The questionnaire was administered two times by two different investigators at an interval of 1 to 3 days for 30 subjects. Choice of this interval was dictated on the one hand by the need for stable clinical status, and on the other hand by the need to avoid memorization of the responses.
1.2.5.3
The validity study
1.2.5.3.1
Face validity
Consideration of face validity was based partially on the appraisal of the committee of experts, and partially on the users’ judgments.
1.2.5.3.2
Content validity
Consideration of content validity was predicated on the appraisal of the committee of experts. In accordance with their experience, the experts appraised the quality of the items in the index by comparing the translated scale with the original version. In addition, internal consistency was assessed by means of the Cronbach alpha coefficient.
1.2.5.3.3
Construct validity
In the absence of a “Gold Standard”, construct validity assessment was based on consideration of the validity of the construct (or external structure), which involves convergent and discriminant validity and consideration of internal structure validity.
External structure (construct) validity: convergent validity was assessed by correlation of the overall index score with the VAS scores pertaining to pain and functional disability of the upper extremity (from 0 to 100 mm) and by study of the correlation of the index with two other functional indexes for the shoulder, that is to say the DASH and the SPADI translated into Arabic through the same method of translation. Discriminant validity was studied by assessment of correlation of the overall index score with the following variables: age, civil status, profession, sports activity, and type of shoulder pathology.
Internal structure validity: factorial analysis followed by orthogonal rotation facilitated consideration of the factorial structure of the scale. The internal consistency of the index and of each factor extracted after the factorial analysis was thoroughly studied.
1.2.5.4
Statistical analysis
The SYSTAT NTS and SPSS programs for Windows were employed in the statistical analysis. Quantitative variables were described through use of means, standard deviation and confidence limits. Qualitative variables were described through use of proportions and percentages.
Interrater concordance (repeatability) was appraised by consideration of the ICC and the Bland and Altman method .
Convergent and discriminant validity were studied by means of the Spearman rank correlation coefficient. In accordance with the value of the coefficient, results were judged excellent with r > 0.91, good with r between 0.71 and 0.9, average with r between 0.51 and 0.7, weak with r between 0.31 and 0.5, very poor or null with r < 0.3.
The factorial structure of the scale was assessed through factorial analysis followed by orthogonal rotation (Varimax). The factorial analysis was brought about in principal components so as to extract the main factors. The factors selected showed a value higher than 1. Internal consistency was studied by means of the Cronbach alpha coefficient and judged satisfactory with alpha greater than 0.7.
The chosen degree of significance was “ P < 0.05”.
1.3
Results
1.3.1
The intermediate scale and preliminary test
Translation of the selected index followed by adaptation of some items led to the establishment of an intermediate scale.
The intermediate scale of our index constituted the subject of a preliminary study; it was completed by 15 persons (ten women and five men) whose average age was 50 years (min. 21; max. 70) of whom eight were illiterate. This step occasioned several linguistic modifications; the terms that seemed difficult for patients to assimilate were replaced by simpler terms; the questions’ meanings nonetheless remained unaltered.
Concepts lacking any equivalent in Tunisian culture were modified in view of adapting them to the local context. Item #5, for example, was changed; washing up on toilets replaced the use of toilet tissue. As was the case with some of the proposed answers, certain verbs, adjectives and nouns used in the items were formulated in dialectical Arabic, and were put in parentheses for explanatory purposes.
The group of patients was satisfied with regard to the pertinence and intelligibility of the questions; the final version of the intermediate scale was consequently elaborated.
1.3.2
Clinical and demographic data used in the series
For our final study, we selected 80 subjects, of whom 63.8% were female, while 52.5% exercised no profession. Sixty-six percent of the subjects had a primary or secondary educational level. Table 1 summarizes the remaining clinical and demographic data.
| Minimum | Maximum | Mean | Standard deviation | |
|---|---|---|---|---|
| Age | 21.0 | 75.00 | 51.42 | 12.7932 |
| VAS pain | 0.00 | 100.0 | 51.31 | 27.1627 |
| VAS disability | 5.0 | 85.00 | 46.81 | 24.2253 |
| ASES score | 0.00 | 90 | 45.64 | 22.99 |
1.3.3
Modifications of the intermediate scale subsequent to study of the series
Following consideration of the series, the intermediate scale was in no way modified; not a single item was withdrawn from the questionnaire. The final ASES version included ten items and a visual analogue scale (VAS) pertaining to pain ( Appendix B ).
1.3.4
Metrological properties of the index
1.3.4.1
Feasibility and acceptability
The mean time taken to fill out the ASES was 2.5 minutes (min. 2; max. 3.5). All the items were satisfactorily acceptable.
1.3.4.2
Interrater concordance
The ICC was 0.969. Interrater concordance (repeatability) was judged excellent ( Table 2 ).
| Measurement 1 of the ASES score | Measurement 2 of the ASES score | |
|---|---|---|
| Means | 54.11 | 53.43 |
| Standard deviation from the mean | 4.61 | 4.32 |
| 95% confidence interval for the mean | [44.67–63.55] | [44.58–62.28] |
| ICC | 0.96 | |
| 95% confidence interval for the ICC | [0.918–0.981] |
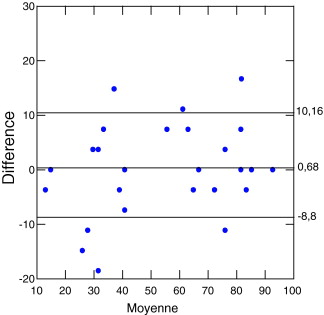
The Bland and Altman method confirmed the questionnaire’s satisfactory repeatability. Indeed, study of the mean differences of the reported scores showed a distribution of data points around zero, plus or minus two standard deviations ( Fig. 1 ).
1.3.4.3
Validity
1.3.4.3.1
Face validity
Since the translated version of the index consisted in the same number of items as the original index, face validity may be deduced from the former; our scale consequently shows satisfactory face validity.
1.3.4.3.2
Content validity
Our scale showed satisfactory homogeneity between the different dimensions. The Cronbach alpha coefficient was 0.813.
1.3.4.3.3
Structure validity
External structure (construct) validity: as regards discriminant validity, we found no correlation between the index and the parameters that were initially considered as discriminant criteria ( Table 3 ). As regards convergent validity, while correlation between the index and functional disability VAS was better than correlation with the pain VAS, the two results were judged average. On the other hand, correlation of the ASES index with the DASH and SPADI indexes was considered good ( Table 4 ). These findings confer satisfactory convergent validity on the ASES.
| Age | Civil status | Profession | Sports activity | Type of shoulder pathology | |
|---|---|---|---|---|---|
| r | −0.143 | −0.045 | 0.109 | 0.171 | 0.184 |
| P | 0.205 | 0.69 | 0.366 | 0.13 | 0.102 |
| DASH | SPADI | VAS disability | VAS pain | ||
|---|---|---|---|---|---|
| ASES score | r | −0.858 | −0.799 | −0.583 | −0.497 |
| P | 0.000 | 0.000 | 0.000 | 0.000 |
Internal structure validity: factorial principal component analysis (PCA) after ASES varimax rotation with regard to the studied population enabled extraction of two factors with a cumulative variance rate of 92.6%. The first factor includes items 3, 4, 7 and 8, while the second factor includes items 1, 2, 5, 6, 9 and 10. The internal consistency of each of the two factors was appraised by the Cronbach alpha coefficient, which was equal to 0.76 for the first component and to 0.54 for the second component ( Table 5 ).
| Component 1 | Component 2 | |
|---|---|---|
| ASES 1 | 0.344 | 0.917 |
| ASES 2 | 0.557 | 0.811 |
| ASES 3 | 0.728 | 0.678 |
| ASES 4 | 0.953 | 0.224 |
| ASES 5 | 0.385 | 0.713 |
| ASES 6 | 0.557 | 0.811 |
| ASES 7 | 0.976 | 0.175 |
| ASES 8 | 0.953 | 0.224 |
| ASES 9 | 0.633 | 0.748 |
| ASES 10 | 0.287 | −0.883 |
1.4
Discussion
This work describes the translation into Arabic and adaptation of the ASES index as well as the study of its metrological qualities.
Subsequent to choice of the index, translation constituted the initial step. When a translation is made into literary Arabic, it may be difficult to use, particularly in a population of illiterate subjects. In our previous studies of the Tunisian population, we showed that 50 to 60% of subjects aged more than 40 years were illiterate . That is why we decided to translate the questionnaires into a simple, nearly dialectical Arabic.
Translation methods are numerous, and have not been standardized. Several difficulties involving translation and linguistic adaptation have been described and pertain mainly to the target languages . Given the fact that strict methodological rules of translation do not exist, our translation procedure was close to that adopted by the International Quality of Life Assessment project (IQOLA).
The problem encountered during this step consisted in finding comprehensible terms in Tunisian dialect. Popular Tunisian dialect is highly rich and varied, in exactly the same manner as are the cultures composing that population (Arab, African and Mediterranean). In cases where literary translation ran the risk of being poorly or not at all understood by an illiterate subject and where a simpler version of literary Arabic was not found, it was decided to at once conserve the literary version and to add, in parentheses, its dialectical equivalent. This choice has already been adopted in several studies and recommended at this stage of translation .
The pretest (preliminary) study allowed us to detect the terms that might be poorly or not at all assimilated by patients, in particular the illiterate. We recommend that the pretest be carried out on a group of illiterate patients from different regions if possible, so as to more closely detect the insufficiencies of the intermediate versions.
As regards concepts that have no equivalent from one country to another, the choice is to totally modify the item so that it fits in with the cultural context . In our own work, we transformed item ASES 5 from “use of toilet tissue” to “washing up on toilets”. In the final analysis, the adaptations performed in our study changed neither the number of items and answers in the original scale, nor the patterns of answers.
The preliminary study is of essential importance. It often leads to new adaptations, and allows for an initial assessment of the scales. Several preliminary studies are at times needed, in order to produce usable indexes .
Consideration of the metrological qualities of our index entailed consideration of its repeatability and validity.
As regards the study of repeatability (interrater concordance), we made use of the “intraclass” correlation and the Bland and Altman method. Association of these methods suffices to judge repeatability . In our study, the ICC was 0.969. Interrater concordance was judged excellent. During validation of the ASES in its original version, the ICC was 0.94 and 0.89 ; in its French and German-language versions, it exceeded 0.90 . The Bland and Altman method confirmed the ICC, and suggested satisfactory repeatability of the Arabic-language version of the index.
The validity study was complicated by the lack of any “Gold Standard” for functional assessment of the shoulder. And so, the study consisted in no less than three steps: face validity, content validity and structure validity.
The length of the Arabic-language version of the ASES was judged acceptable. The average time taken to fill it out was 2.5 minutes, as opposed to 3 minutes in its original version . Acceptability was good as regards all the items.
The internal consistency study by means of the Cronbach alpha factor showed good internal consistency (alpha coefficient at 0.81). In its original version, the Cronbach alpha coefficient was 0.86 ; in its French and German versions, it was higher than or equal to 0.90 . For some authors, a translation methodically carried out ensures the content validity and the face validity of the questionnaire .
Evaluation of the structure validity is consequently of the utmost importance. It is assessed by convergent validity, discriminant validity and analysis of the validity of the internal structure. As regards convergent validity, we have found the mean correlations between on the one hand our VAS pain and VAS functional disability and on the other hand the other functional indexes for the shoulder, namely the DASH and the SPADI, to be good to excellent. These correlations also provide our index with good convergent validity. Correlations between the ASES score and these two indexes were good ( r > 0.7) in the different translated versions . Discriminant validity was likewise good.
Factorial analysis in PCA after Varimax rotation enabled extraction of two components that could not be explained; that said, alpha Cronbach figures show them to possess a certain internal consistency.
1.5
Conclusion
The approach followed in our study allowed us to achieve in easy literary Arabic a version of the ASES index for functional evaluation of the shoulder that was adapted to the Tunisian population.
This version is repeatable, and its structure validity is satisfactory. Study of sensitivity to change shall be the subject of upcoming work. Our index assesses functional shoulder disability and is correlated to the intensity of pain and the extent of functional disability. Other studies will be needed in order to verify the validity of this version in other Arabic-language populations.
Conflict of interest statement
None.
2
Version française
2.1
Introduction
Le retentissement fonctionnel peut être très important dans la pathologie de l’épaule, touchant les capacités professionnelles, mais souvent aussi les activités de la vie quotidienne. L’examen clinique est certes important lors de l’évaluation de la pathologie de l’épaule mais il ne permet pas de connaître le retentissement de cette affection sur la vie quotidienne du malade. L’évaluation fonctionnelle prend ainsi une place primordiale dans la pathologie de l’épaule, car un des buts essentiel de tout traitement dans cette pathologie est d’améliorer la fonction .
Plusieurs indices et tests ont été élaborés pour l’évaluation de la fonction du membre supérieur, certains sont spécifiques des atteintes de l’épaule, d’autres sont utilisés dans les pathologies touchant de façon plus globale le membre supérieur.
Parmi ces indices on cite le Disabilities of the Arm, Shoulder and Hand Scale (DASH) qui est un autoquestionnaire d’évaluation du membre supérieur non spécifique d’une pathologie . Il comprend 30 items répartis en quatre domaines : symptômes, fonction physique, fonction sociale et fonction psychologique. Le DASH a de bonnes qualités métrologiques dans sa version originale en anglais. Il a été traduit et adapté en français, en chinois, en allemand, en grec, en japonais, en coréen, en espagnol, en russe, en norvégien, en suédois et en turque . Il existe une version courte du DASH (le quickDASH) qui comprend 11 items parmi les 30 items du DASH et qui a été validée en langue originale avec des qualités métrologiques satisfaisantes. Le quickDASH a de bonnes qualités métrologiques et peut être utilisé au lieu du DASH dans l’évaluation des pathologies du membre supérieur .
Le Shoulder Pain And Disability Index (SPADI) est un autoquestionnaire spécifique de l’épaule qui est composé de 13 items évaluant les domaines physiques et sociaux : cinq items pour la douleur et huit items pour l’incapacité . Il a de bonnes qualités métrologiques. C’est l’un des indices les plus utilisés dans les études cliniques.
Parmi les indices spécifiques, on cite aussi l’« American Shoulder and Elbow Surgeons Evaluation Form » (ASES) qui est largement utilisé dans l’évaluation fonctionnelle des pathologies de l’épaule ( Annexe 1 ). Cet indice est souvent utilisé dans l’évaluation postopératoire des pathologies de la coiffe des rotateurs, des épaules instables et de l’articulation acromioclaviculaire .
L’objectif de notre étude était de traduire en arabe l’ASES et d’étudier ses qualités métrologiques dans une population tunisienne.
2.2
Matériels et méthodes
2.2.1
L’indice
L’ASES est un autoquestionnaire de dix items. Ces items correspondent respectivement à la possibilité de lancer un ballon avec une seule main, de dormir sur l’épaule atteinte confortablement, de s’habiller seul, de se laver le dos, de faire la toilette, de laver les cheveux seul, de porter 10 kg au-dessus de l’épaule, d’atteindre une étagère au-dessus de la tête, d’exécuter les tâches quotidiennes au long de la journée et de pratiquer les activités sportives habituelles.
Chaque item comporte quatre niveaux de réponses cotés de 0 à 3 : la réponse 0 correspond à une impossibilité de faire la tâche ; la réponse 1 correspond à la possibilité de faire la tâche avec difficulté modérée ; la réponse 2 correspond à la possibilité de faire la tâche avec difficulté minime et la réponse 3 correspond à la possibilité de faire la tâche sans difficulté.
L’interprétation du score global passe par une addition des valeurs des dix questions qui permettent d’obtenir un score total qui va de 30 (aucune gêne fonctionnelle) à 0 (gêne maximale). Une règle de trois : score total (ST) divisé par 0,3 (ST/0,3), permet ensuite de ramener le score à une échelle de 0 à 100, d’interprétation plus intuitive : 100 (aucune gêne fonctionnelle) à 0 (gêne maximale) .
La traduction en arabe de l’indice a été effectuée selon la méthode de traduction/contre-traduction et a été réalisée de façon indépendante par trois traducteurs bilingues. Les traductions ont été ensuite soumises à la critique de trois experts (deux médecins de médecine physique et un traducteur professionnel) pour tester leur intelligibilité et pour apporter les adaptations nécessaires aussi bien sur le plan linguistique que culturel. La synthèse des différentes traductions a permis d’obtenir une version arabe définitive très proche de la version originale et rédigée dans un langage littéraire simple, facile à comprendre même par des illettrés.
Une contre-traduction de l’arabe vers l’anglais a été faite par deux autres traducteurs professionnels non avertis des propriétés recherchées de l’instrument puis ces deux contre-traductions ont été confrontées à la version originale.
2.2.2
L’adaptation du questionnaire
Lorsqu’un concept n’a pas d’équivalent dans la culture tunisienne, le choix a été de modifier totalement l’item en question pour l’adapter au contexte culturel. La version finale a été revue par le comité d’experts, afin d’apporter les adaptations nécessaires. Les difficultés de traduction, les diversités culturelles, les équivalences conceptuelles ainsi que les différences linguistiques ont été bien mises en évidence lors de cette étape.
2.2.3
Prétest
L’échelle traduite a été testée sur un groupe de 15 personnes de la population générale (prétest) afin de vérifier l’acceptabilité du questionnaire, en évaluant la compréhension des questions et le nombre de réponses manquantes. À la fin de cette étape, une échelle intermédiaire a été obtenue.
2.2.4
Étude de la série
2.2.4.1
Patients
Ont été inclus dans notre étude des patients âgés de 20 à 80 ans ayant une des pathologies abarticulaires de l’épaule suivantes : tendinopathie, rupture de la coiffe des rotateurs ou épaule bloquée. Le diagnostic reposait sur un examen clinique bien orienté de l’épaule complété par une échographie en suspicion d’une atteinte de la coiffe des rotateurs. Ont été exclus de l’étude tous les patients ayant des états pathologiques aiguës, une arthrite inflammatoire ou infectieuse de l’épaule, une pathologie tumorale ou osseuse de l’épaule, une pathologie du coude, du poignet ou de la main, une épaule paralytique, des désordres psychiatriques graves ou débilite mentale et un refus de participation à l’étude. Les données cliniques et démographiques ont été recueillies pour tous les patients.
2.2.4.2
Méthodes
Les questions ont été énoncées mot à mot comme elles sont rédigées. L’investigateur ne pouvait pas changer les mots mais avait la possibilité de répéter les questions. Les questions non compréhensibles ont été éliminées. Une analyse statistique des réponses a été par la suite effectuée afin de sélectionner les questions des échelles finales. La distribution des réponses a été analysée pour chaque item ; un item est éliminé si sa distribution n’est pas bonne (effet plafond ou effet plancher).
Le coefficient de corrélation intraclasse (CCI) a été utilisé pour la reproductibilité de chaque item ; une question a été éliminée si son CCI est inférieur à 0,7.
À la fin de cette étape, une version finale a été obtenue.
2.2.5
Évaluation des propriétés métrologiques de la version finale
2.2.5.1
Faisabilité et acceptabilité
La faisabilité et l’acceptabilité des échelles ont été appréciées par le nombre de données manquantes pour chaque item, par la compréhension des questions posées et par le temps nécessaire pour répondre au questionnaire.
2.2.5.2
Étude de la reproductibilité
Le questionnaire a été administré à deux reprises par deux investigateurs différents avec un intervalle d’un à trois jours pour 30 sujets. Le choix de cet intervalle a été dicté par la nécessité de la stabilité du statut clinique, d’une part, et l’absence de mémorisation des réponses, d’autre part.
2.2.5.3
Étude de la validité
2.2.5.3.1
La validité d’apparence
L’étude de la validité d’apparence a été basée, d’une part, sur l’appréciation du comité d’experts et, d’autre part, sur le jugement des utilisateurs.
2.2.5.3.2
La validité de contenu
L’étude de la validité de contenu s’est appuyée sur l’appréciation du comité d’experts. En fonction de leur expérience, les experts ont apprécié la qualité des items de l’indice en comparant l’échelle traduite à sa version originale. Par ailleurs la cohérence interne a été évaluée par le coefficient alpha de Cronbach.
2.2.5.3.3
La validité de structure
En absence de « Gold Standard », l’évaluation de la validité de structure a reposé sur l’étude de la validité de structure externe ou de construit (qui comporte la validité convergente et divergente) et l’étude de la validité de structure interne.
La validité de structure externe ou de construit : la validité de convergence a été évaluée par la corrélation du score global de l’indice avec les scores de l’EVA douleur et incapacité fonctionnelle du membre supérieur (de 0 à 100 mm), ainsi que l’étude de la corrélation de l’indice avec deux autres indices fonctionnels de l’épaule le DASH et le SPADI traduits en arabe par la même méthode de traduction. La validité de divergence a été étudiée par l’évaluation de la corrélation du score global de l’indice avec les variables suivantes : l’âge, l’état civil, la profession, l’activité sportive et le type de la pathologie de l’épaule.
La validité de structure interne : une analyse factorielle suivie d’une rotation orthogonale a permis l’étude de la structure factorielle de l’échelle. La cohérence interne de l’indice ainsi que celle de chaque facteur extrait après l’analyse factorielle ont été étudiées.
2.2.5.4
Analyse statistique
Les programmes SYSTAT NTS et SPSS pour windows ont été utilisés pour l’analyse statistique. Les variables quantitatives ont été décrites en utilisant les moyennes, l’écart-type et les limites. Les variables qualitatives ont été décrites en utilisant des proportions et des pourcentages.
La reproductibilité a été appréciée par l’étude du CCI , ainsi que la méthode de Bland et Altman .
Les validités de convergence et de divergence ont été étudiées à l’aide du coefficient de corrélation de Spearman. En fonction de la valeur du coefficient, les résultats ont été qualifiés d’excellents si r > 0,91, bons si r entre 0,71 et 0,9, moyens si r entre 0,51 et 0,7, faibles si r entre 0,31 et 0,5, très mauvais ou nuls si r < 0,3.
La structure factorielle de l’échelle a été évaluée par analyse factorielle suivie d’une rotation orthogonale (Varimax). L’analyse factorielle a été réalisée en composantes principales pour extraire les facteurs principaux. Les facteurs retenus avaient une valeur supérieure à 1. La cohérence interne a été étudiée par le coefficient alpha de Cronbach, elle a été jugée bonne si alpha supérieur à 0,7.
Le degré de signification retenu était « p < 0,05 ».
2.3
Résultats
2.3.1
L’échelle intermédiaire et prétest
La traduction de l’indice choisi suivie de l’adaptation de certains items a permis d’obtenir une échelle intermédiaire.
L’échelle intermédiaire de notre indice a fait l’objet d’une pré-étude et a été complétée par 15 personnes (dix femmes et cinq hommes) d’âge moyen 50 ans (min. 21 ; max. 70) dont huit sont illettrées. Cette étape a donné lieu à certaines modifications linguistiques : les termes qui paraissaient difficiles à assimiler par les patients ont été échangés par d’autres plus simples tout en conservant le sens des questions.
Les concepts qui n’ont pas d’équivalents dans la culture tunisienne ont été modifiés afin de les adapter au contexte culturel. L’item n o 5 a été modifié : se laver sur les toilettes a remplacé l’usage du papier toilette. Quelques verbes, adverbes et noms ont été utilisés directement en arabe dialectal aussi bien dans les items que dans les réponses possibles, et ils ont été mis entre parenthèses à titre explicatif.
La pertinence et l’intelligibilité des questions ont été jugées bonnes par ce groupe de patients. Ainsi la version finale de l’échelle intermédiaire a été obtenue.
2.3.2
Données cliniques et démographiques de la série
Nous avons retenu pour l’étude finale 80 sujets, 63,8 % étaient de sexe féminin, 52,5% étaient sans profession. Soixante-six pour cent des sujets avaient un niveau primaire ou secondaire. Le Tableau 1 résume le reste des données cliniques et démographiques.
Related posts:
 Self care programs and multiple sclerosis: Physical therapeutics treatment – literature review
Neuromuscular fatigue in healthy muscle: Underlying factors and adaptation mechanisms
Risk assessment analysis of the future technical unit dedicated to the evaluation and treatment of motor disabilities
The Prevention of Foot Ulceration in Diabetic Patients
Psychosocial Factors in Chronic Pain in the Dysvascular and Diabetic Patient
Elbow Arthroscopy
Self care programs and multiple sclerosis: Physical therapeutics treatment – literature review
Neuromuscular fatigue in healthy muscle: Underlying factors and adaptation mechanisms
Risk assessment analysis of the future technical unit dedicated to the evaluation and treatment of motor disabilities
The Prevention of Foot Ulceration in Diabetic Patients
Psychosocial Factors in Chronic Pain in the Dysvascular and Diabetic Patient
Elbow Arthroscopy
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


