Transforaminal Lumbar Interbody Fusion
Introduction
Transforaminal lumbar interbody fusion (TLIF) first described in 1982
Enables fusion of spinal segment anteriorly and posteriorly through single posterior procedure; eliminates morbidity, complications of anterior fusion
Can access disk space through single unilateral posterior approach, preserving contralateral lamina and spinous process, creating larger surface area for posterolateral fusion
Exposes neural foramen for direct decompression, eliminates need to retract thecal sac, reducing risk of incidental durotomy, neural injury
Intervertebral disk space ideal for obtaining bony fusion due to compressive forces of anterior column and blood supply provided by prepared end plates
In lumbar spine, 80% of mechanical load transmitted through vertebral body, 20% through posterior elements; in posterolateral fusion, fusion bed under tensile forces; in interbody fusion, fusion surface under compression
TLIF combined with posterolateral instrumentation and fusion achieves fusion rates greater than 90% and clinical outcomes comparable to anterior lumbar interbody fusion with posterolateral instrumentation and fusion
Patient Selection
Indications
TLIF ideal for treating lumbar spine deformity, degenerative disk disease; interbody fusion restores disk space height and lordosis, indirectly decompressing neural foramen and improving sagittal balance
Isthmic spondylolisthesis (grades I and II)
Foraminal intervertebral disk herniations and recurrent disk herniations
Degenerative disk disease causing mechanical back pain with or without radiculopathy
Postlaminectomy spondylolisthesis
Postlaminectomy kyphosis
Lumbar coronal or sagittal plane deformities
Contraindications
Severe osteopenia
Bleeding disorders
Relatively contraindicated in active local or systemic infection
Preoperative Imaging
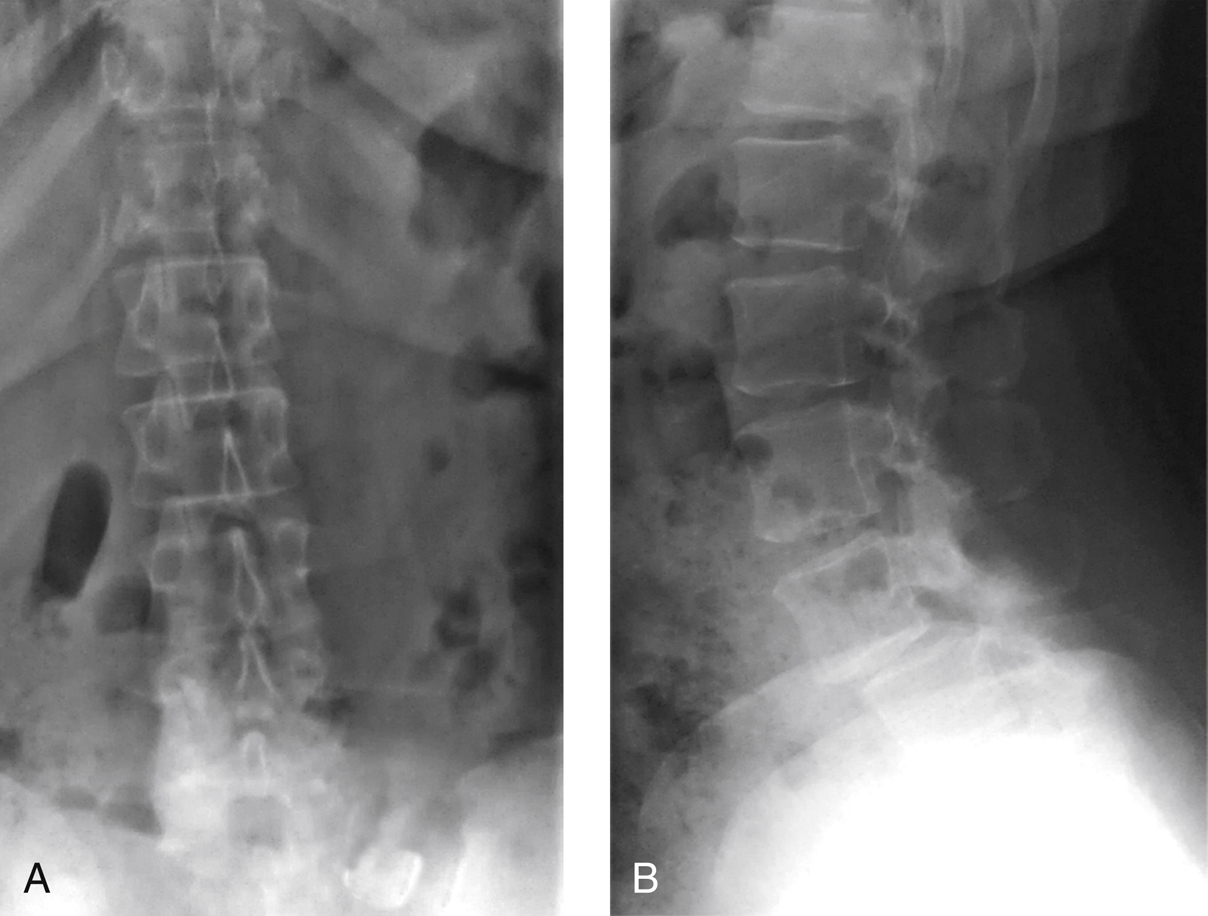
Figure 1Preoperative AP (A) and lateral (B) radiographs show L4-L5 spondylolisthesis in a 54-year-old woman who presented with reports of worsening back pain and lower extremity radiculopathy.
Preoperative AP and lateral radiographs (Figure 1)
CT/MRI
Procedure
Room Setup/Patient Positioning
Prone position on Jackson table
Pad bony prominences; free abdomen of compression to relieve intra-abdominal pressure
Place neuromonitors on lower extremities in lumbar dermatomal distribution
Anesthesiologist keeps patient in hypotensive state to help reduce blood loss
Special Instruments/Equipment/Implants
Pedicle screw system
Structural interbody spacer options: titanium cages, polyetheretherketone cages, structural machined allograft, poly-L/d-lactide resorbable spacer
Bone graft materials
C-arm
Neuromonitoring equipment
Bipolar cautery, straight osteotomes, Kerrison and Leksell rongeurs, straight and curved curets and pituitaries, disk space shavers, disk space dilators, disk space trials, and high-speed burr
Surgical Technique
Open Transforaminal Lumbar Interbody Fusion
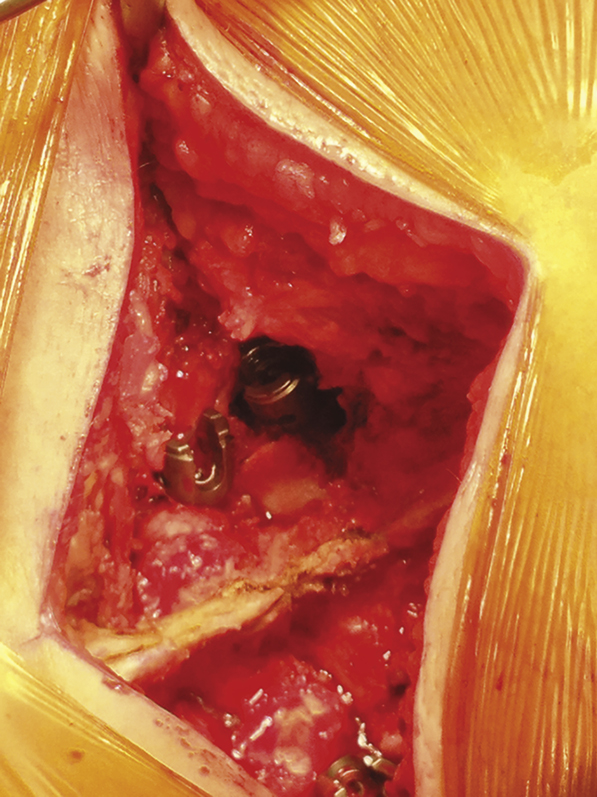
Figure 2Intraoperative photograph shows the transforaminal lumbar interbody fusion window created to access the disk space.
Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


