CHAPTER 12 Tibial Tubercle Transfer
The goal of patellofemoral stabilization surgery is central, tracking of the patella in the femoral trochlea. If stable tracking can be achieved using nonoperative means such as core stability physical therapy, and bracing, surgery should be avoided. The caregiver should also rule out retinacular1,2 or articular3,4 pain causing the knee to give way. A thorough history and examination,5 using pain diagrams6 as needed, is central to accurate diagnosis and appropriate surgical planning. Unfortunately, many patients with recurrent patellar instability require some form of stabilization to function adequately in work and daily life, particularly in more vigorous activities. This is particularly important because chronic lateral patellofemoral articular overload may eventually cause joint breakdown.7 Debate continues regarding the evolution of trochlea dysplasia,8,9 but it is likely that chronic lateral facet overload from lateral patellar tracking10 may contribute to or cause deficiency of lateral trochlear containment of the patella.
It must be considered that balanced patellar tracking with optimal load distribution across the joint is best for patients and presumably minimizes risk of eventual cartilage deterioration and arthritis. Therefore, balanced tracking is of paramount importance. Multiple factors are involved in patellar tracking, including femoral version, tibial version, articular geometry, lower extremity kinematic function, muscle imbalance, foot and ankle mechanics, ligamentory balance of the knee, varies, valgus, body habitus, and posture. Some of these are correctable by nonoperative measures and should therefore be addressed before considering surgery.11 Certainly, an articular lesion causing symptoms of giving way may be mistaken for patellar instability and should be treated appropriately, whether by simple débridement12 or articular resurfacing.13–18
Procedures such as trochleoplasty and femoral and tibial derotation may be appropriate in rare patients but carry risks that many surgeons and patients find unacceptable. Therefore, traditional patellofemoral stabilization, using lateral release, medial retinacular restoration (medial patellofemoral ligament [MPFL] imbrication or reconstruction), and/or medial tibial tubercle transfer remain mainstays of patellofemoral stabilization. Lateral release19–22 has been used widely in the past but has little relevance as an isolated procedure for patients with patellar instability23 and can cause medial patellar instability24 when used extensively or inappropriately.
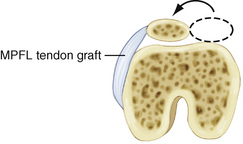
Restoration of patellofemoral balance by MPFL–medial capsule imbrication, often with release of a lateral retinaculum that has become adaptively tight, is desirable, particularly because it is known that the injured MPFL does heal,25 albeit elongated, in most patients. Sometimes, a tendon graft needs to be added to ensure adequate medial retinacular–MPFL support of the patella,26 but this should be done selectively, when less invasive surgery is judged to be insufficient. Many patients with less serious instability are happy to undergo a smaller procedure with the knowledge that another procedure might be needed in the future. This is occasionally preferable to the alternative risk of surgical complication from a more major surgical intervention. In any case, however, it is important to consider that the MPFL is an important restraint to lateral patellar instability27–29; be prepared to restore or reconstruct it selectively once adequate patellar tracking alignment had been ensured. Most important in this type of surgery is to avoid excessive patellofemoral joint loading, because the MPFL is a posteriorly oriented structure (Fig. 12-1). Tibial tubercle transfer is the best way to restore proper tracking of the patella in the trochlea in many cases, after which retinacular balance, including the MPFL, can be restored by imbrication or tendon graft reconstruction but without exerting force on the patella. Following tibial tubercle transfer balancing of the extensor mechanism, however, MPFL restoration is often unnecessary, because it usually adapts over time.
TREATMENT
Indications
In patients with more serious lateral patellar tracking, the medial-lateral distance30 between the tibial tuberosity and trochlear groove (TTTG) is often 15 to 20 mm or more. A well-done axial radiograph at 45 degrees of knee flexion31 and a precise lateral32 radiograph are extremely important in determining the resting position of the patella with respect to the trochlea. The patient with prominent J tracking and disability related to serious lateral patellar tracking will often benefit most from medial transfer of the tibial tubercle.33,34 This is a compensatory procedure that does not correct all the underlying structural problems; however, a medial tibial tubercle transfer yields functional stabilization of the patellofemoral joint quickly and without exerting a posteromedial pull vector on the patella. Tibial tubercle transfer yields balanced patellofemoral tracking, the possibility of immediate range of motion after surgery, and permanent stability when properly and accurately performed.
Tibial tubercle transfer can also unload the distal patella by adding obliquity to the cut behind the tibial tubercle (anteromedial tibial tubercle transfer), thereby lifting up and unloading the distal and lateral patellar articulating surfaces. These are frequently fragmented and/or painful in the patient with chronic lateral patellar tracking.35–40
As the lateral and distal patella manifest evidence of degenerative cartilage related to excessive lateral pressure, anteromedial tibial tubercle transfer becomes more important for redistribution of contact forces on the patella and for enhanced stability and joint preservation. Long-term results of anteromedial tibial tubercle transfer have been very good in properly selected patients with lateral and distal patellar articular damage.40,41 Medial patellofemoral ligament reconstruction is not as likely to help these patients and involves some risk of chronic pain if a fragmented distal medial patella receives added load following medial capsule ligamentous reconstruction.
Nonetheless, retinacular balancing in conjunction with tibial tubercle transfer can be helpful and sometimes necessary. In particular, when there is trochlear dysplasia,42

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


