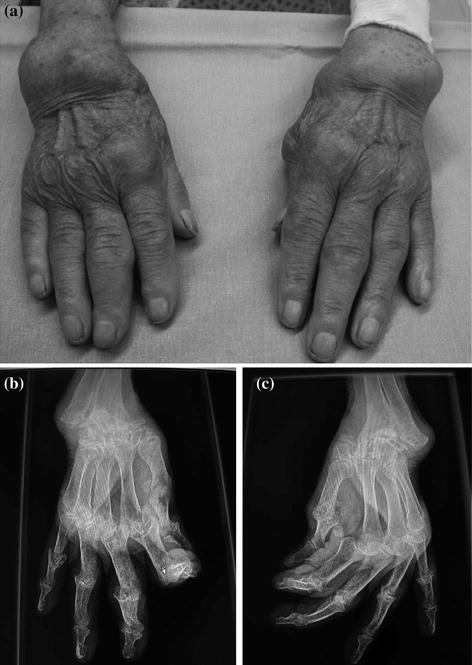
Fig. 3.2
A posterior photograph of patient with rheumatoid arthritis hands (a), note axial deviation of the wrist and clearer observed as seen in X-ray of the right (b) and left (c) wrist [13]
In conjunction with the pathomechanics of the RA, there are cascade of events behind it. The disease process commences by mainly affecting the soft tissues including the adjacent articular cartilage (chondrolysis) then followed by the hard tissues (bone resorption), thus resulting in severe deformities [12, 13] of the joint. To efficiently examine the severity of the RA deformities, previous reports have introduced several classifications according to their own reliable approaches. Larsen et al. classification used radiologic changes for scoring system with the basis of 5 grades, in which the degree of joint and cartilage destructions used as the primary indicators (Table 3.1) [12, 14]. Combination between radiologic findings and therapeutic options were used in the Wrightington classification, with the basis up to four grades (Table 3.2) [13, 15]. Simmen and Huber on the contrary established a classification method purely based on the natural course of the disease, without considering any radiologic inflammatory destruction [12, 16]. This classification distinguished the courses into three types. Table 3.3 provides information on these three classifications of RA.
Larsen score | Radiographic changes |
|---|---|
0 | Normal joint, no changes |
1 | Osteoporosis and swelling |
2 | Joint space narrowing and erosion |
3 | Significant erosion, moderate destruction |
Score | Radiographic finding | Therapy |
|---|---|---|
1 | Osteoporosis, cysts, erosion | Synovectomy |
2 | Carpal Instability | Soft tissue stabilization/partial arthrodesis |
3 | Destruction, subluxation | Arthroplasty/arthrodesis |
4 | Severe radial destruction | Arthrodesis |
Type | Natural course of the disease |
|---|---|
I | Also known as ankylosing type, where spontaneous fusion of the wrist as the indicator |
II | It comes together with arthritic and degenerative changes. This also known as osteoarthritic type showing both the osteoporosis as well as subchondral sclerosis which affects stabilization |
III | The wrist with progressive disintegration and instability (luxation, progredient bone loss and mutilation) can be categorized under this disintegrative type. There are two subtypes: IIIa with more ligamentous instability IIIb with complete loss of carpal anatomy due to marked destruction of the bone |
There are three main characteristics of the wrist affected by RA: cartilage destruction, synovial proliferation and ligamentous laxity [10, 17]. Cartilage destruction of thinning was occurred due to cytochemical action, which resulting in degradation of existing cartilages and inhibition of new cartilage formation [17]. The synovial proliferation may cause bone erosion with sharp edges which might lead to tendon rupture [10, 18]. Ligamentous laxity caused by stretching attributed to synovial expansion, results in ulnar translation and carpal supination. The pathological process begins with inflammation of the synovial, affects commonly at the ulnar side of the wrist joint [10, 12]. It then spreads to adjacent area of the wrist including the radiocarpal joint. The neighbouring tissues which consist of the cartilages, ligaments and tendons degenerate subsequently. In severe cases, tendon rupture occurs with a consequence of kinematic changes of the joint, resulting in disruption of the periarticular bones and the articular surfaces [9, 19]. On the whole, these three symptoms have critically caused degeneration of both soft tissues and bones, hence eventually mutilated and unstable wrist joint.
Related posts:





Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


