Chapter 7. The wrist and hand
SUMMARY
Repetitive strain injury and work-related upper limb disorder have done much to focus the clinician on the differential diagnosis and causative factors of pain in the wrist and hand.
This chapter takes a pragmatic approach to the identification of specific lesions and suggests localized treatment, which may form a component of overall management. The detailed but relevant anatomy that forms a basis for accurate treatment is presented. Treatment for individual lesions is discussed, with emphasis on the application of principles to less commonly encountered lesions.
ANATOMY
Inert structures
The distal radioulnar joint is a pivot joint between the head of the ulna and the ulnar notch of the radius. Mechanically linked to the superior radioulnar joint, it is responsible for the movements of pronation (85°) and supination (90°).
A triangular fibrocartilaginous articular disc closes the distal radioulnar joint inferiorly and is the main structure uniting the radius and ulna (Palastanga et al 2006). It lies in a horizontal plane, its apex attaching to the ulnar styloid and its base to the lower edge of the ulnar notch of the radius. The disc articulates with the lunate when the hand is in ulnar deviation. It adds to the stability of the joint and acts as an articular cushion for the ulnar side of the carpus, absorbing compression, traction and shearing forces but being prone to degenerative changes (Livengood 1992, Rettig 1994, Wright et al 1994, Steinberg & Plancher 1995).
The movements of pronation and supination rotate the radius around the ulna. Supination is stronger, hence the thread of nuts and screws which are tightened by supination in right-handed people.
There are two rows of carpal bones; on the palmar aspect, from the radial to the ulnar side they are:
scaphoid, lunate, triquetral, pisiform
trapezium, trapezoid, capitate, hamate.
The carpal bones all articulate with their neighbours, except pisiform, which is a separate bone situated on the front of the triquetral. The intercarpal joints are all supported by intercarpal ligaments.
The wrist joint proper is a biaxial, ellipsoid joint between the distal end of the radius and the articular disc, and the proximal row of carpal bones. However, the so-called wrist joint complex includes the midcarpal joint and has mobility as well as stability, which is important for the function of the hand. Movements are extension (passive, 85°), flexion (passive, 85°), ulnar deviation (passive, 45°) and radial deviation (passive, 15°). The close packed position of the wrist joint is full extension.
The joints are surrounded by a fibrous capsule, lined with synovial membrane and reinforced by collateral ligaments. Both collateral ligaments pass from the appropriate styloid process to the carpal bones on the medial and lateral side of the carpus. A fibrocartilaginous meniscus projects into the joint from the ulnar collateral ligament.
The metacarpophalangeal joints are ellipsoid; the interphalangeal joints are hinge joints. Both are supported by palmar and collateral ligaments and the extensor tendons and digital expansions support the dorsal surfaces of the joints. Flexor tendons are contained within fibrous sheaths which have thickened areas known as pulleys which may provide a restriction, producing ‘trigger finger’ (see p. 175). At the wrist and in the hand, the tendons are contained within synovial sheaths (Standring 2009).
The flexor retinaculum, a strong fibrous band, creates a fibro-osseous passage, the carpal tunnel, through which pass the flexor tendons of the digits, the median nerve and vessels. The flexor retinaculum has four points of attachment: the pisiform and hook of hamate medially and the tuberosity of the scaphoid and ridge of trapezium laterally. Its attachment onto the trapezium splits to form a separate compartment for the tendon of flexor carpi radialis. The median nerve enters the carpal tunnel deep to palmaris longus. It shares its compartment of the carpal tunnel with nine tendons comprising the four tendons of flexor digitorum superficialis and the four tendons of flexor digitorum profundus, and flexor pollicis longus. On leaving the carpal tunnel it supplies the thenar muscles before dividing into four or five digital branches.
The trapeziofirst-metacarpal joint (first carpometacarpal joint) is a saddle joint with a loose articular capsule and extensive joint surfaces giving it a wide range of movement. The first metacarpal has been rotated medially for the movement of opposition.
Flexion and extension occur in a plane parallel to the palm of the hand, while abduction and adduction occur in a plane at right angles to the palm of the hand (Fig. 7.1 a–d).
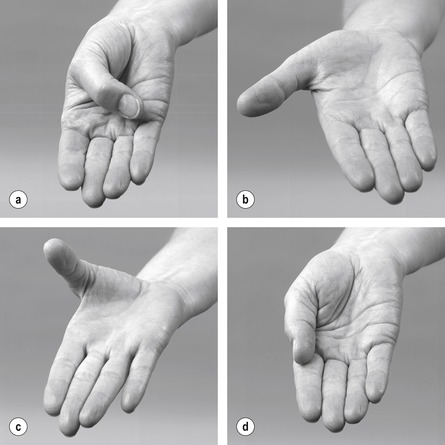 |
| Figure 7.1 Movements of the metacarpophalangeal joint of the thumb: (a) flexion; (b) extension; (c) abduction; (d) adduction. |
The close packed position of the trapeziofirst-metacarpal joint is strong opposition, when great force is transmitted to the joint. The functionally opposed thumb is subjected to compressive stresses which make the joint vulnerable to degenerative osteoarthrosis.
The radial artery passes under abductor pollicis longus and extensor pollicis brevis, crossing the snuffbox obliquely towards the first dorsal interosseous muscle. Its position should be acknowledged so that it can be avoided when injecting the trapeziofirst-metacarpal joint.
Contractile structures
Flexor carpi radialis (median nerve C6–C7) is the most lateral superficial flexor tendon. It passes through its own fibro-osseous compartment on the lateral side of the carpal tunnel, to insert into the base of the second and third metacarpals.
Palmaris longus (median nerve C7–C8) passes over, not under, the flexor retinaculum, to attach to the distal part of the flexor retinaculum and the palmar aponeurosis.
Flexor digitorum superficialis (median nerve C7–C8, T1) lies medial to palmaris longus, but is not as visible because it lies on a slightly deeper plane. In the carpal tunnel the four tendons are contained within the same synovial sheath, with tendons to the third and fourth fingers lying superficial to those to the second and fifth. The tendons divide to provide a passage for flexor digitorum profundus, before continuing on to insert either side of the middle phalanx.
Flexor carpi ulnaris (ulnar nerve C7–C8) is the most medial superficial flexor tendon and can be easily traced onto its insertion into pisiform. The tendon sends slips onwards as the pisohamate and pisofifth-metacarpal ligaments. The pisohamate ligament converts the space between pisiform and the hamate into a tunnel (tunnel of Guyon) for the passage of the ulnar vessels and nerves.
Flexor pollicis longus (median nerve C8, T1) passes through the lateral side of the carpal tunnel and inserts into the palmar aspect of the base of the distal phalanx of the thumb.
Flexor digitorum profundus (medial part supplied by the ulnar nerve; lateral part supplied by the median nerve C8, T1) divides into four tendons which lie deep to flexor digitorum superficialis in the carpal tunnel. They pass through tunnels created by superficialis and attach to the distal phalanx of each finger.
The lumbricals are four small muscles which arise from the flexor digitorum profundus tendons and pass to the radial side of the dorsal digital expansions of each finger. With attachments that link flexor and extensor tendons, they function by flexing the metacarpophalangeal joints and extending the interphalangeal joints. The first two lumbricals are supplied by the median nerve, the third and fourth by the ulnar nerve, C8, T1.
Extensor carpi radialis longus (radial nerve C6–C7) and extensor carpi radialis brevis (posterior interosseous nerve C7–C8) pass deep to the tendons of abductor pollicis longus and extensor pollicis brevis, under the extensor retinaculum, to attach to the radial side of the base of the second and third metacarpals respectively.
Extensor digitorum (posterior interosseous nerve C7–C8) divides into four tendons which pass under the extensor retinaculum to insert into the dorsal digital expansions of the fingers.
Extensor digiti minimi (posterior interosseous nerve C7–C8) inserts into the dorsal digital expansion of the little finger.
Extensor carpi ulnaris (posterior interosseous nerve C7–C8) lies in a groove between the head of the ulna and the styloid process, under the extensor retinaculum. It attaches to the medial side of the base of the fifth metacarpal.
Abductor pollicis longus and extensor pollicis brevis (posterior interosseous nerve C7–C8) become tendinous and superficial in the lower forearm where they cross the tendons of extensor carpi radialis longus and brevis at the intersection point, a site of potential friction. They occupy the same synovial sheath in the first compartment of the extensor retinaculum and form the lateral border of the anatomical snuffbox. The abductor inserts into the base of the first metacarpal and the extensor into the base of the proximal phalanx. Because of its position, abductor pollicis longus has been considered both anatomically and functionally a radial deviator of the wrist (Elliott 1992a).
Extensor pollicis longus (posterior interosseous nerve C7–C8) deviates around the ulnar side of the dorsal tubercle of the radius, to pass to the base of the distal phalanx of the thumb. It forms the medial border of the anatomical snuffbox.
Extensor indicis (posterior interosseous nerve C7–C8) joins the ulnar side of the extensor digitorum tendon, passing to the index finger.
The dorsal interossei (ulnar nerve C8, T1) are four bipennate muscles arising from adjacent sides of the metacarpal bones and inserting into the dorsal digital expansion and base of the proximal phalanx of the appropriate finger. They are responsible for abducting the fingers from the midline of the middle finger.
The palmar interossei (ulnar nerve C8, T1) are four smaller muscles originating from the palmar aspect of the metacarpal bones and inserting into the dorsal digital expansions of the appropriate finger. They are responsible for adducting the fingers towards the middle finger.
GUIDE TO SURFACE MARKING AND PALPATION
Palmar aspect (Fig. 7.2)
Look for three creases (not distinct in everyone) on the palmar aspect of the lower forearm. The distal wrist crease joins pisiform and the tubercle of the scaphoid, the bones at the heel of the hand (Backhouse & Hutchings 1990), marking the proximal border of the flexor retinaculum. The middle crease joins the two styloid processes, marking the position of the wrist joint line, while the proximal crease (if present) marks the proximal extent of the flexor tendon sheaths.
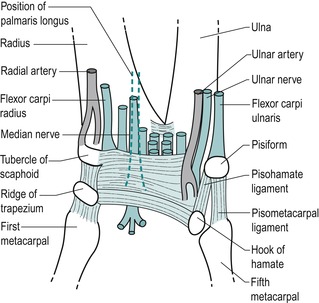 |
| Figure 7.2 Palmar aspect of the wrist showing position of the flexor retinaculum, its adjacent tendons and nerves. |
Consider the position of the bones which make up the two rows of carpal bones (Fig. 7.3). From the radial to the ulnar side, an easy way to remember the order is:
| simply learn the parts | scaphoid, lunate, triquetral, pisiform |
| that the carpus has | trapezium, trapezoid, capitate, hamate |
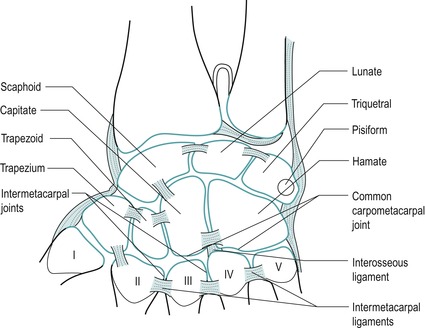 |
| Figure 7.3 Bones of the hand. From Anatomy and Human Movement by Palastanga N, Field D and Soames R 2006. Reprinted by permission of Elsevier Ltd. |
Palpate pisiform, the pea-shaped sesamoid bone, which lies at the base of the hypothenar eminence, giving insertion to flexor carpi ulnaris.
Move a thumb approximately 1.5 cm distally and diagonally from pisiform, in the direction of the index finger. Lying roughly in line with the ring finger is the hook of hamate. Palpate deeply and tenderness will confirm its presence.
Radially deviate the wrist to make the tuberosity of the scaphoid more prominent. It lies at the base of the thenar eminence, close to the tendon of flexor carpi radialis. Move a thumb from the tuberosity of the scaphoid, diagonally and distally approximately 1 cm, to lie in line with the index finger, and feel the ridge of the trapezium through the bulk of the thenar eminence. It is best felt with the wrist joint in extension and is tender to deep palpation.
Joining the four points described above – pisiform, hook of hamate, tuberosity of scaphoid and ridge of trapezium – gives the position of the flexor retinaculum, which is approximately the size of your thumb when placed horizontally across the proximal palm (Fig. 7.2).
Identify the superficial forearm flexor tendons as they cross the palmar aspect of the wrist from the radial to ulnar side. Flexor carpi radialis is the most lateral tendon. Palmaris longus passes over the flexor retinaculum and can be brought into prominence by opposing the thumb and little finger with the wrist flexed. Flexor digitorum superficialis, lying in a deeper plane, may not be readily palpable, but flexor carpi ulnaris can be followed down to its insertion onto the pisiform.
Palpate for the radial pulse on the palmar aspect of the lower radius lateral to flexor carpi radialis. The ulnar pulse can be palpated on the lower ulna, lateral to flexor carpi ulnaris.
Consider the position of the median nerve as it enters the carpal tunnel deep to palmaris longus. If palmaris longus is absent, oppose the thumb and little finger and the midline crease produced gives the position of the median nerve.
Dorsal aspect (Fig. 7.4)
Pronate the forearm and the head of the ulna can be seen as a rounded elevation in the distal forearm. Palpate to the ulnar side of the head and feel the tendon of extensor carpi ulnaris in the groove between the head of the ulna and the styloid process.
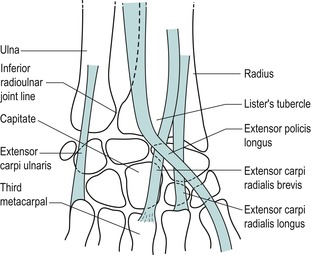 |
| Figure 7.4 Dorsal aspect of the wrist. |
Palpate the inferior radioulnar joint line, which lies approximately 1.5 cm laterally from the ulnar styloid. Confirm its presence by passively gliding the head of the ulna on the radius and feeling the joint line.
On the lower end of the radius, palpate the dorsal tubercle (of Lister) lying roughly in line with the index finger. The tubercle is grooved on either side by the passing tendons. Extensor carpi radialis longus and brevis pass on its lateral side, while extensor pollicis longus passes on its medial side before taking a 45° turn laterally, where it can be traced to its insertion into the base of the distal phalanx of the thumb.
The capitate is the largest carpal bone and is roughly the size of the patient’s thumb nail. It is wider dorsally and is roughly peg-shaped. It is situated in the centre of the carpus, articulating mainly with the third metacarpal distally, the trapezoid laterally, the hamate medially and the concavity formed by the scaphoid and lunate proximally (Steinberg & Plancher 1995, Standring 2009). To locate the position of the capitate, run your finger proximally down the shaft of the third metacarpal with the wrist in slight flexion and drop over the end into the shallow depression.
Place the wrist in flexion with the thumb relaxed to allow the tendon of extensor pollicis longus to fall out of the way and to expose the base of the metacarpals. Now palpate the insertions of extensor carpi radialis longus and brevis onto the radial side of the base of the second and third metacarpals respectively. The extensor carpi radialis brevis is probably the easier of the two to feel. Palpate the insertion of extensor carpi ulnaris onto the medial side of the base of the fifth metacarpal.
Lateral aspect (Fig. 7.5)
Pronate the forearm and make a fist. The fleshy elevation seen at the distal end of the radius is formed by the musculotendinous junctions of abductor pollicis longus and extensor pollicis brevis as they wind around the lower radius, crossing over the tendons of extensor carpi radialis longus and brevis at the intersection point.
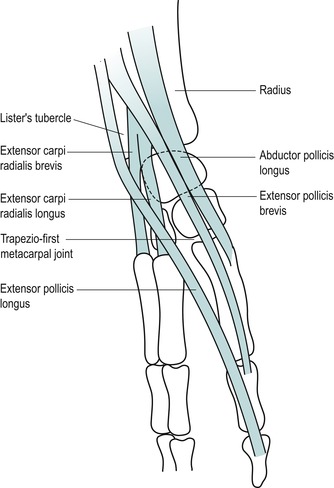 |
| Figure 7.5 Tendons on the lateral aspect of the wrist. |
Locate the anatomical snuffbox (by extending the thumb) which is bordered by the tendons of abductor pollicis longus and extensor pollicis brevis laterally and by extensor pollicis longus medially. Palpate the radial styloid at the proximal end of the anatomical snuffbox and the trapeziofirst-metacarpal joint at the distal end.
Locate the tendons of abductor pollicis longus and extensor pollicis brevis; sometimes a V-shaped gap may be appreciated between the two.
Move the wrist into ulnar deviation and the scaphoid can be palpated distal to the radial styloid; it moves with the hand, whereas the radial styloid does not. The scaphoid can be grasped between your thumb posteriorly in the base of the snuffbox and your index finger anteriorly.
Move distally to palpate the trapezium lying between the scaphoid and the base of the first metacarpal.
Palpate the trapeziofirst-metacarpal joint line by running a thumb down the shaft of the first metacarpal into the anatomical snuffbox. Flex and extend the joint to check its location.
Palpate the first dorsal interosseous in the web between index finger and thumb; it can be made more prominent by resisting abduction of the index finger.
COMMENTARY ON THE EXAMINATION
Observation
Before proceeding with the history, a general observation of the patient’s face, posture and gait will alert the examiner to serious abnormalities or injuries. The painful hand may be held in an antalgic position, resting with the fingers parallel to each other and in a degree of flexion, the thumb in a neutral position. Possibly, the arm swing may be absent from the gait pattern and the hand held stiffly against the side or across the body. Difficulty with fine movement may be observed during undressing, indicating a problem with dexterity.
History (subjective examination)
The age, occupation, sports, hobbies and lifestyle of the patient may give an indication of the cause and a possible diagnosis, since most problems in the lower forearm involve arthritis, trauma or overuse. Mobile phone texting and the use of hand-held gaming devices have joined the more traditional causative factors of overuse of scissors and keyboard, etc. The specific activities required in an occupation should be explored to expose the precise movements required of the upper limb, often repetitively for several hours a day. Racquet sports, golf, hockey, etc. can all give rise to symptoms in the wrist and hand resulting from the impact forces and positioning of the upper limb.
The site of pain is usually well localized by the patient, with little spread, since these are peripheral joints and structures lying at the end of their respective dermatomes, with little scope for reference. The presence of paraesthesia or any apparent reference of pain may suggest a more proximal lesion, and all proximal joints must be examined, including the cervical spine. A fractured scaphoid gives localized pain and point tenderness in the anatomical snuffbox, while X-ray investigation may not show evidence of the fracture for several weeks (Livengood 1992).
The onset of the symptoms may be due to trauma, overuse or arthritis. If the onset is traumatic in nature, the possibility of fracture should be eliminated. Frequently, a direct injury involving a fall on the outstretched hand may cause fracture of the scaphoid or subluxation of the capitate or lunate bones, and may also cause a traumatic arthritis with soft tissue swelling and contusion. Indirect injury may also occur from a rotational force or maximal effort in racquet sports (Rettig 1994).
Most injuries at the wrist and hand develop from repetitive overuse. Tendinopathy may result from frequent overstretching or unaccustomed activity. An overuse syndrome occurs when the level of repeated microtrauma exceeds the tissue’s ability to adapt (Rettig 1994). Tensional overload or abnormal shear stresses can cause microtrauma at any point in the musculotendinous or ligamentous unit. The syndromes of carpal tunnel and de Quervain’s (see p. 171 & 174) may be associated with more proximal lesions, such as nerve entrapment or lesions of the cervical spine.
A hyperextension injury to the thumb is a relatively common sporting injury, producing a traumatic arthritis in either the trapeziofirst-metacarpal joint or the metacarpophalangeal joint. This may occur in skiing (‘skier’s thumb’) or sports which involve ball-catching, e.g. volleyball, netball or goal-keeping in football.
Arthritis in the hand may be inflammatory, degenerative or traumatic. Rheumatoid arthritis is common in the smaller joints and therefore readily affects the joints of the wrist and hand where deformity is characteristic; it is usually bilaterally symmetrical. Any synovial space can be involved, including the tendon sheaths and bursae, as well as the joints. Juvenile chronic arthritis has less symmetrical joint involvement than adult rheumatoid arthritis.
Primary degenerative osteoarthrosis affects the trapeziofirst-metacarpal joints and the distal interphalangeal joints more readily. These joints are subjected to stress in the functional position and are used through all extremes of range, predisposing them to primary arthritis. Secondary degenerative osteoarthrosis can affect any joint.
The duration of symptoms indicates the stage of the lesion in the inflammatory process. Overuse syndromes have a gradual onset with symptoms present for many months. Rheumatoid arthritis and acute episodes of degenerative osteoarthrosis tend to have periods of remission and exacerbation while traumatic lesions may be of fairly short duration.
The symptoms and behaviour need to be considered. The behaviour of the pain indicates the nature of the lesion, with mechanical lesions eased by rest and aggravated by activity. Overuse lesions are worsened by repetition of the mechanism of trauma. The nature of the pain is also important: is it localized or vaguely diffuse, deep or superficial, sharp, burning, aching, constant or intermittent, getting worse or better, or staying the same?
The other symptoms described by the patient could include paraesthesia. An accurate description of these associated symptoms is relevant to the source of pressure or nerve entrapment. The distribution of pins and needles and whether or not they possess edge and/or aspect helps to determine their origin. Stiffness of the hand may be relevant to arthritis or ligamentous lesions and it is therefore appropriate to know the daily pattern of the symptoms. Heat, coldness, sweating, dryness and other sensory changes may also be relevant, suggesting the vasomotor changes of Raynaud’s disease or reflex sympathetic dystrophy.
An indication of past medical history, other joint involvement and medications will establish whether contraindications to treatment techniques exist. As well as past medical history, establish any ongoing conditions and treatment. Explore other previous or current musculoskeletal problems with previous episodes of the current complaint, any treatment given and the outcome of treatment.
Inspection
Fracture or dislocation commonly occurs with a fall on the outstretched hand and shows obvious bony deformity and swelling. Subluxation, e.g. of the capitate, may be seen as a bump on the dorsum of the hand with the wrist in flexion.
Deformities of the fingers are commonly associated with rheumatoid arthritis or may result from forced hyperextension injuries, as in wicket keepers, for example. If an extensor tendon is avulsed or torn from the distal phalanx, a mallet finger occurs with flexion of the distal interphalangeal joint. This can be associated with sporting injuries or may simply occur if the finger is forcibly caught, while making the bed, for example. A bony swelling of the distal interphalangeal joint is a characteristic deformity known as a Heberden’s node, associated with primary degenerative osteoarthrosis.
Degenerative osteoarthrosis of the trapeziofirst-metacarpal joint produces a capsular pattern which may draw the thumb into a position of flexion and medial rotation with bony osteophytes obvious at the base of the thumb. Dupuytren’s contracture is a deformity with contraction of the palmar fascia, causing flexion of principally the ring and little fingers. Clubbed fingers may be indicative of systemic disease.
Colour changes, which may indicate circulatory involvement, should be further investigated by palpating for the arterial pulses. The fingers, in particular, can give clues to serious underlying pathology and the colour and shape of the fingers and nails should be noted. Bruising may be apparent, resulting from direct trauma, and may be associated with abrasions on the palm due to a fall on the outstretched hand.
Muscle wasting may be obvious in the flattening of the thenar muscles, producing the ape-like hand with the thumb moving back in line with the other fingers. This indicates involvement of the median nerve in the carpal tunnel or possibly cervical nerve root pressure. Similarly, the ulnar nerve or lower cervical nerve root compression involves the hypothenar eminence, and if the intrinsic muscles are involved a claw hand develops. Involvement of the radial nerve affects the wrist extensors and produces a dropped wrist.
Swelling indicates active inflammation and the wrist may be fixed in the mid-position due to the presence of a joint effusion. Contusions with swelling are due to direct trauma. Excessive friction of the skin causes callus and blister formation, e.g. rowing and gymnastics. Ganglia are mucus-filled cysts, which are commonly seen around the wrist, particularly on the dorsum of the hand. They are common between the second and fourth decades of life (Smith & Wernick 1994) and if symptomatic may be burst or require surgical excision. Rheumatoid nodules may be present.
Palpation
Since these are peripheral joints, palpation for signs of activity is conducted. Temperature changes are assessed and heat indicates an active inflammation, while cold may indicate circulatory problems (Fig. 7.6). It may be appropriate to palpate the ulnar and/or radial pulse (Fig. 7.7). Synovial thickening is usually palpated on the dorsum of the wrist (Fig. 7.8). Swelling is usually observed around the wrist where it may be fusiform, unilateral or bilateral. Other swellings, such as nodules or ganglia, can be palpated to assess whether they are hard or soft.
 |
| Figure 7.6 Palpation for heat. |
 |
| Figure 7.7 Palpation for radial pulse. |
 |
| Figure 7.8 Palpation for synovial thickening. |
State at rest
Before any movements are performed, the state at rest is esta-blished to provide a baseline for subsequent comparison.
Examination by selective tension (objective examination)
The suggested sequence for the objective examination will now be given, followed by a commentary including the reasoning in performing the movements and the significance of the possible findings. Comparison should always be made with the other side.



 Get Clinical Tree app for offline access
Get Clinical Tree app for offline access

Inferior radioulnar joint


Wrist joint
• Passive flexion (Fig. 7.11)
Related posts:






Stay updated, free articles. Join our Telegram channel
Full access? Get Clinical Tree