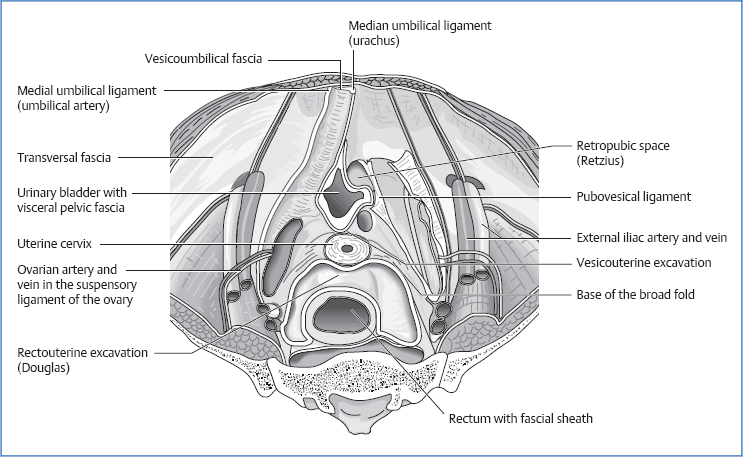
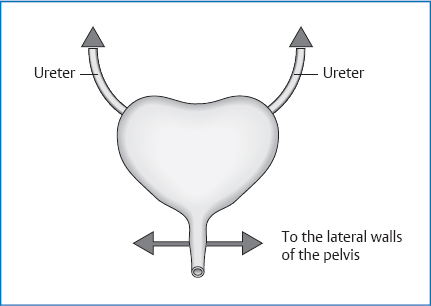
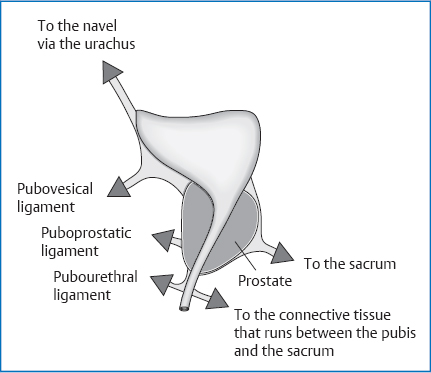
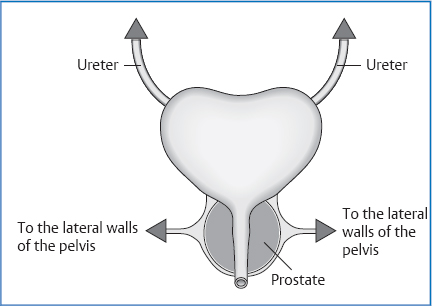
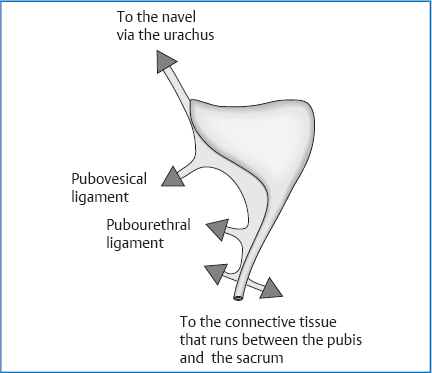
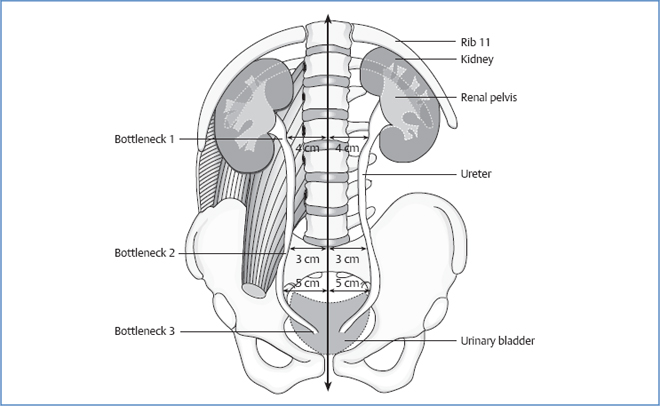
15 The Urinary Bladder The bladder’s normal capacity lies at 500mL, but strong urinary urgency occurs already with 300 mL. In patients with voiding dysfunctions after surgery, up to 2000mL can collect. The urinary bladder is located in the lesser pelvis behind the symphysis. An empty bladder does not extend with its superior pole beyond the symphysis; a full bladder can be palpated up to 3 cm above the symphysis. Superior Anterior Inferior Posterior Lateral. Peritoneum, runs into the broad ligament of the uterus. Fig. 15.1 Topography of the female lesser pelvis. Fig. 15.2 Fascial attachments of the organs in the lesser pelvis. Fig. 15.3 Topography of the male lesser pelvis. Superior Anterior Inferior. Prostate gland. Posterior Fig. 15.4 Ligaments of the bladder, frontal view. Fig. 15.5 Ligaments of the bladder, sagittal view. Lateral Retropubic space (Retzius space): Located between the pubic bone/abdominal wall and the urinary bladder, bordered caudally by the pubovesical ligament and medially by the median umbilical ligament. Fig. 15.6 Ligaments of the bladder, side view, in the male body. Fig. 15.7 Ligaments of the bladder, in the male body (view from the front). Branches of the internal iliac artery, e.g.: Internal and external iliac nodes. Maximal time: 3–5p.m. Minimal time: 3–5a.m. For basic information, see page 34. The ureter is 25–30cm long and approximately 5mm thick. There are three physiologic bottlenecks where kidney stones are most likely to get impacted: The ureter runs caudal on top of the psoas major, passes across the bifurcation of the common iliac artery (left) or the external iliac artery (right) as it enters the lesser pelvis, and then descends further caudally along the lateral wall of the pelvis near the peritoneum. Fig. 15.8 Location of the ureter. Roughly at the level of the ischiadic spine, it changes its course medially and anteriorly in the direction of the urinary bladder. Slightly above the seminal vesicle, it reaches the posterior lateral wall of the bladder, where it is crossed by the vas deferens. Here, the vas deferens lies closer to the peritoneum than the ureter. Continuing on, the ureter crosses the bladder diagonally from posterolat-eral to anteromedial. Roughly at the level of the ischiadic spine, it changes its course medially and anteriorly in the direction of the urinary bladder. It initially lies in the base of the broad ligament of the uterus, and then it is crossed by the uterine artery. In its continued path, it proceeds at a distance of about 1–2cm away from the supravaginal part of the uterine cervix. Right in front of the urinary bladder, it lies on top of the anterior and lateral vaginal vault. Entry into the urinary bladder takes place diagonally, as in the male body. See “Location”; in addition: Fig. 15.9 Topographic relationships of the ureter. The arterial supply is provided by branches of the arteries in its vicinity: The urinary bladder moves together with the sacrum and uterus: during inhalation posteriorly and superiorly and during exhalation anteriorly and inferiorly. Another movement results when the bladder is filled with urine and then voided. During the expiratory phase, we see a movement postero-superiorly, and during the inspiratory phase in the opposite direction. Urine reaches the bladder in portions. The peristaltic contraction of the ureter opens and closes the opening of the ureter. The ureter penetrates the urinary bladder diagonally. As a result, the internal pressure of the bladder keeps the entrance of the ureter closed except for during peristaltic waves. This mechanism prevents a reflux of urine. The pelvic floor becomes limp, and the bladder consequently shifts lower, its neck assuming a funnel shape. Urine enters the urethra up to the inner sphincter, the detrusor muscle of the bladder contracts (innervated parasympathetically), and the funnel shape is reinforced. The sphincter opens. The urethra muscles and the external sphincter become limp. To conclude micturition, the pelvic floor as well as the internal and external sphincter contract, and the neck of the bladder loses its funnel shape. Definition. Infection of the upper urinary tract due to pathogenic organisms. Causes. Highly virulent organisms coinciding with a weakened state of defense. Precipitating factors include: Clinical
Anatomy
 Anatomy of the Urinary Bladder
Anatomy of the Urinary Bladder
General Facts
Location
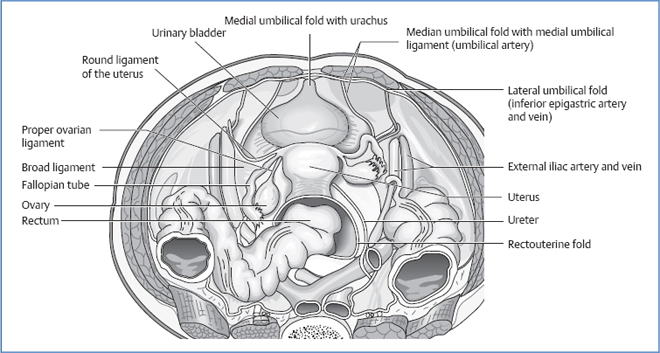
Topographic Relationships
Female Pelvis
 peritoneum
peritoneum
 small intestinal loops
small intestinal loops
 uterus (depending on location)
uterus (depending on location)
 pubis
pubis
 peritoneum
peritoneum
 when bladder is full: anterior abdominal wall
when bladder is full: anterior abdominal wall
 uterine cervix
uterine cervix
 vagina
vagina
 urethra
urethra
 pelvic floor (levator ani)
pelvic floor (levator ani)
 obturator internus
obturator internus
 uterine cervix and isthmus
uterine cervix and isthmus
 vagina
vagina
 ureter
ureter
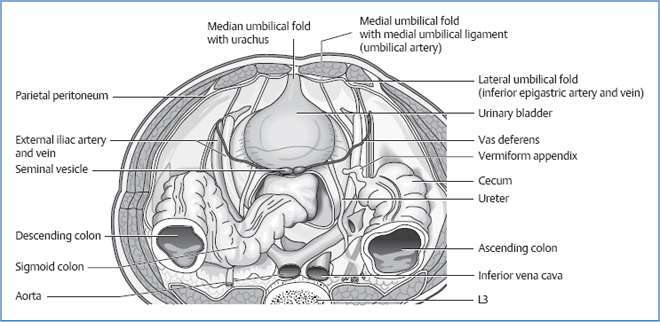
Male Pelvis
 peritoneum
peritoneum
 intestinal loops
intestinal loops
 pubis
pubis
 peritoneum
peritoneum
 when bladder is full: anterior abdominal wall
when bladder is full: anterior abdominal wall
 vas deferens
vas deferens
 seminal vesicle
seminal vesicle
 rectum
rectum
 ureter
ureter
 peritoneum
peritoneum
 small intestinal loops
small intestinal loops
 peritoneum
peritoneum
 levator ani
levator ani
 obturator internus
obturator internus
Attachments/Suspensions
 peritoneum (anterior, lateral, and in men also posterior attachment)
peritoneum (anterior, lateral, and in men also posterior attachment)
 median umbilical ligament (with urachus)
median umbilical ligament (with urachus)
 medial umbilical ligament (obliterated umbilical artery)
medial umbilical ligament (obliterated umbilical artery)
 pubovesical ligament (with muscle fibers from the bladder), corresponds to the puboprostatic ligament
pubovesical ligament (with muscle fibers from the bladder), corresponds to the puboprostatic ligament
 connective tissue of the lesser pelvis
connective tissue of the lesser pelvis
Circulation
Arterial
 inferior vesical artery
inferior vesical artery
 internal pudendal artery
internal pudendal artery
 obturator artery
obturator artery
Venous
 vesical venous plexus (anastomoses to the prostatic and vaginal venous plexus)
vesical venous plexus (anastomoses to the prostatic and vaginal venous plexus)
 internal iliac vein
internal iliac vein
Lymph Drainage
Innervation
 sympathetic nervous system from L1 to L2 via the intermesenteric plexus and hypogastric nerves to the inferior hypogastric plexus and vesical plexus
sympathetic nervous system from L1 to L2 via the intermesenteric plexus and hypogastric nerves to the inferior hypogastric plexus and vesical plexus
 sacral parasympathetic nervous system (S2–S4) via the inferior hypogastric plexus and vesical plexus
sacral parasympathetic nervous system (S2–S4) via the inferior hypogastric plexus and vesical plexus
Organ Clock
Organ–Tooth Interrelationship
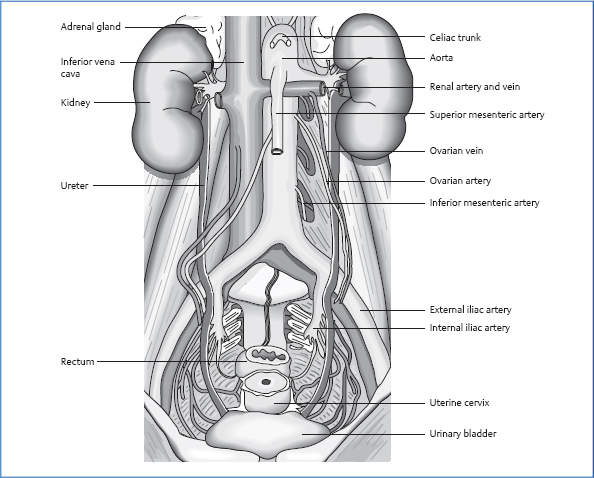
 Anatomy of the Ureter
Anatomy of the Ureter
General Facts
Location
Continued Path in the Male Body
Continued Path in the Female Body
Topographic Relationships
 peritoneum
peritoneum
 psoas fascia
psoas fascia
 genitofemoral nerve
genitofemoral nerve
 inferior vena cava (right)
inferior vena cava (right)
 duodenum (right)
duodenum (right)
 testicular/ovarian vessel
testicular/ovarian vessel
 right colic artery
right colic artery
 ileocolic artery
ileocolic artery
 inferior mesenteric artery or left colic artery
inferior mesenteric artery or left colic artery
 root of the mesentery
root of the mesentery
 root of the sigmoid mesocolon
root of the sigmoid mesocolon
Attachments/Suspensions
 adipose capsule of the kidney
adipose capsule of the kidney
 peritoneum
peritoneum
 retro- and extraperitoneal connective tissue
retro- and extraperitoneal connective tissue
Circulation
Arterial
 renal artery
renal artery
 abdominal aorta
abdominal aorta
 testicular/ovarian artery
testicular/ovarian artery
 common iliac artery
common iliac artery
 internal iliac artery
internal iliac artery
 inferior vesical artery
inferior vesical artery
 uterine artery
uterine artery
Venous
 testicular/ovarian vein
testicular/ovarian vein
 internal iliac vein
internal iliac vein
 vesical plexus
vesical plexus
Lymph Drainage
 internal/communal/external iliac nodes
internal/communal/external iliac nodes
 lumbar nodes
lumbar nodes
 renal lymph nodes
renal lymph nodes
Innervation
 sympathetic nervous system from T10 to L1 via the lesser and lowest splanchnic nerves and the lumbar splanchnic nerves 1 and 2 to the celiac plexus, aorticorenal ganglion, renal plexus, and posterior renal ganglion
sympathetic nervous system from T10 to L1 via the lesser and lowest splanchnic nerves and the lumbar splanchnic nerves 1 and 2 to the celiac plexus, aorticorenal ganglion, renal plexus, and posterior renal ganglion
 vagus nerve (via the celiac plexus)
vagus nerve (via the celiac plexus)
 sacral parasympathetic system (S2–S4) via the superior hypogastric plexus to the renal plexus
sacral parasympathetic system (S2–S4) via the superior hypogastric plexus to the renal plexus
Movement Physiology according to Barral
Mobility
Motility
Physiology
Mechanism of Bladder Filling and Voiding
Micturition
Pathologies
Symptoms that Require Medical Clarification
Cystitis
 stricture of the urinary tract, e.g., prostatic hyperplasia
stricture of the urinary tract, e.g., prostatic hyperplasia
 vesicoureteral reflux
vesicoureteral reflux
 neurogenic disturbance of bladder voiding
neurogenic disturbance of bladder voiding
 calculi
calculi
 diabetes mellitus
diabetes mellitus
 immunosuppressive therapy
immunosuppressive therapy
 dysuria
dysuria
 pollakiuria
pollakiuria
 subfebrile temperatures
subfebrile temperatures
Osteopathic Practice
Cardinal Symptoms
Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


