(1)
Department of Orthopedic Surgery Academic Medical Centre, University of Amsterdam, Amsterdam, The Netherlands
Abstract
A high percentage of residual complaints is reported after an acute lateral ankle ligament rupture. At long-term follow-up, 30–40 % of patients report restrictions. Residual complaints are related to the initial pathology. On the lateral side, the sequela is caused by traction forces resulting in avulsions. On the medial side of the ankle/foot, compression forces result in cartilage damage. This chapter describes the mechanism and sequela of supination trauma at the various locations in the ankle/foot. It also points out which lesions can be treated.
A high percentage of residual complaints is reported after an acute lateral ankle ligament rupture.
On the lateral side, the sequela is caused by traction forces resulting in avulsions.
On the medial side of the ankle/foot, the compression forces result in cartilage damage.
After a supination trauma, 60 % of patients have pain on the anteromedial aspect or posteromedial aspect of the ankle.
10.1 Introduction
A high percentage of residual complaints is reported after an acute lateral ankle ligament rupture. At long-term follow-up, 30–40 % of patients report restrictions. Development of residual complaints after supination trauma is related to the initial pathology (see Table 10.1 and Fig. 10.1).
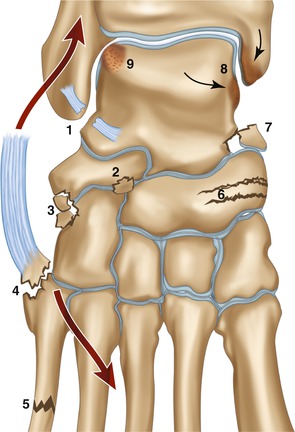
Table 10.1
Sequela of supination trauma in relation to initial pathology
Lateral | Ruptured lateral ankle ligaments—chronic instability |
Ligament avulsion fibula tip | |
Syndesmotic rupture | |
Lateral talar process fracture | |
Anterolateral | Sinus tarsi syndrome |
Cuboid avulsion | |
Fractured fifth metatarsal | |
Anteromedial | Navicular bone fracture |
Cartilage damage medial malleolus/medial talar facet | |
Posteromedial | Ligament avulsion |
Damaged deltoid ligament/ossicle/calcification | |
Posterior | Posterior talar facet fracture/os trigonum impingement |
Posterolateral | Longitudinal rupture peroneus brevis tendon |
Ankle joint | (Osteo)chondral damage |
Synovitis/scar tissue |
Fig. 10.1
Supination results in distraction forces on the lateral side (fat arrows) and compression (thin arrows) on the medial side. On the lateral side, this can lead to a rupture of the ankle ligaments (1), avulsion of the anterior calcaneal process (2), avulsion at the calcaneocuboid joint (3), avulsion of the peroneus brevis at the metatarsal fifth bone (4), or a metatarsal shaft fracture (5). On the medial side, due to compression, this can lead to a navicular fracture (6), an anteromedial compression injury of the talus (7), or a compression injury between medial malleolus and medial talar facet (8). Finally as a result of a supination trauma in 3–5 % of the cases, a cartilage lesion of the lateral talar dome can occur (9)
10.2 Lateral Sequela
The incidence of chronic mechanical instability after acute ankle ligament rupture is reported to be less than 10 % (Karlsson et al. 1988). More than half of these patients will regain satisfactory functional stability after a supervised rehabilitation program based on peroneal muscle strengthening and coordination training (Kerkhoffs et al. 2002). Some patients have residual complaints due to an avulsion which has resulted in a nonunion of the avulsion. A neglected rupture of the syndesmotic ligaments can result in chronic syndesmotic instability. The incidence of subtalar instability is probably overestimated. A lateral talar process fracture can often only be detected by CT scan (Fig. 10.2). Arthroscopy can play a role in the detection of syndesmotic laxity, in shrinkage of the ATFL in case of laxity, and in resection of a small lateral talar process fragment.
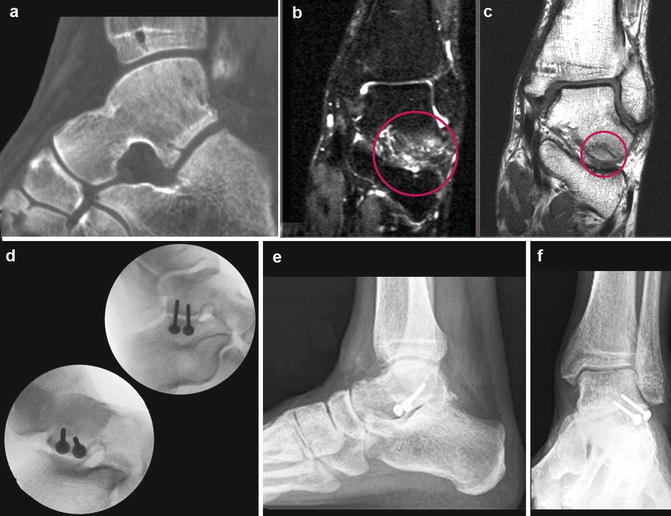
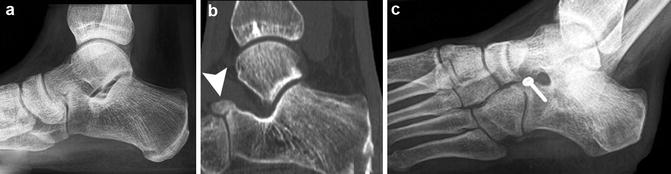
Fig. 10.2
(a) CT scan showing pseudarthrosis of a lateral talar process (snowboarders injury). (b) MRI T2 shows bone edema as a result of this pseudarthrosis of the lateral talar process. (c) MRI T1 shows the fracture of the anterolateral talar process. (d, e, f) Situation after screw fixation
10.3 Anterolateral Sequela
The incidence of sinus tarsi syndrome after supination trauma is unknown.
Patients with a sinus tarsi syndrome in 70 % report an inversion injury as the cause (Klein et al. 1993; Taillard et al. 1981; Oloff et al. 2001). In some patients, there is a fracture of the anterior calcaneal process as a cause of sinus tarsi syndrome (Fig. 10.3). Avulsion fractures of the cuboid joint have no consequences. A fracture of the fifth metatarsal can result in a painful nonunion when neglected (Fig. 10.4) (Kerkhoffs et al. 2012). Arthroscopy can play a role in resection of a nonunion of an anterior calcaneal process fragment.