10 The Pancreas The pancreas is 14–18cm long and weighs 70–80g. It is a gland with exocrine and endocrine features. The pancreas is a secondarily retroperitoneal organ. It lies on the median line roughly at the level L1 – L2, with the head lower than the tail: the axis of the body is inclined toward the upper left approximately 30° to the horizontal line. The accessory pancreatic duct, if present, enters the duodenum 2–3 cm above the major duodenal papilla. Fig. 10.1 Topographic relationships of the pancreas. Maximal time: 9–11 a.m. Minimal time: 9–11 p. m. For basic information, see page 34. Due to the good fascial anchoring in the retroperitoneal space, it is impossible to detect a separate mobility. Nevertheless, the movements of the neighboring organs and the diaphragm cause pushing and pulling on the pancreas. With a hand that rests on the projection of the pancreas on the abdomen (fingers pointing to the tail, thenar lies above the head), we can detect a wave from the heel of the hand to the fingertips during exhalation. During inhalation, the wave runs in the opposite direction. The pancreas is a gland with exocrine and endocrine features. The endocrine parts, the islets of Langerhans, are distributed throughout the entire pancreas with accumulations in the body and tail. The cells in the islets of Langerhans produce the hormones that are responsible for regulating blood sugar: insulin, glucagon, and somatostatin. Insulin is synthesized in the β cells of the islets of Langerhans (approximately 2mg/day) and lowers the blood sugar level by making the cell wall of each body cell permeable to glucose. In addition, insulin assists in the uptake of different amino acids into the cell. In the liver, it initiates a variety of metabolic processes: Glucagon is produced in the a cells of the islets. It is the “insulin antagonist”: by promoting glycogenolysis and gluconeogenesis in the liver, it raises the blood sugar level. The δ cells synthesize this hormone. It suppresses the release of insulin and glucagons, and decreases digestive activity by reducing intestinal peristalsis and inhibiting the secretion of digestive juices. Its function is to maintain the glucose level as much as possible. The exocrine gland part of the pancreas secretes juice into the pancreatic duct. As a result of its activity, approximately 1–1.5 L of “abdominal saliva” thus reaches the duodenum per day. This secretion consists of: The enzymes of this “abdominal salivajanu” are not yet activated in the pancreas. It is only after contact with bile or the enterokinase in the duodenal juice that they are activated and begin working. If this activation takes place in the pancreas, it results in autodigestion and the symptoms of acute pancreatitis. Definition. Inflammation of the pancreas with disturbance of exocrine and endocrine functions. Rare causes include: Definition. Chronic inflammation of the pancreas is characterized by persistent or recurrent pain with usually irreversible morphologic changes in the pancreatic parenchyma and functional disturbances in the pancreas. Rare causes include: When approximately 90% of pancreatic tissue is destroyed, we see steatorrhea as a sign of maldigestion, as well as symptoms of fat-soluble vitamin deficiency (night blindness, clotting disorders, osteomalacia). Definition. Malignant tumor of the pancreas, usually originating in the epithelium of the duct system. Causes. Unknown genesis. Under discussion are alcohol, nicotine, and coffee consumption as predisposing factors. Clinical. No early symptoms.
Anatomy
General Facts
Division
 head of pancreas with the uncinate process
head of pancreas with the uncinate process
 body of pancreas
body of pancreas
 tail of pancreas
tail of pancreas
 pancreatic duct (Wirsung)
pancreatic duct (Wirsung)
 accessory pancreatic duct (Santorini)
accessory pancreatic duct (Santorini)
Location
Topographic Relationships
 duodenum
duodenum
 L2–L3 (head of pancreas), covered by the right crus of the diaphragm
L2–L3 (head of pancreas), covered by the right crus of the diaphragm
 common bile duct
common bile duct
 aorta
aorta
 inferior vena cava
inferior vena cava
 left renal vein
left renal vein
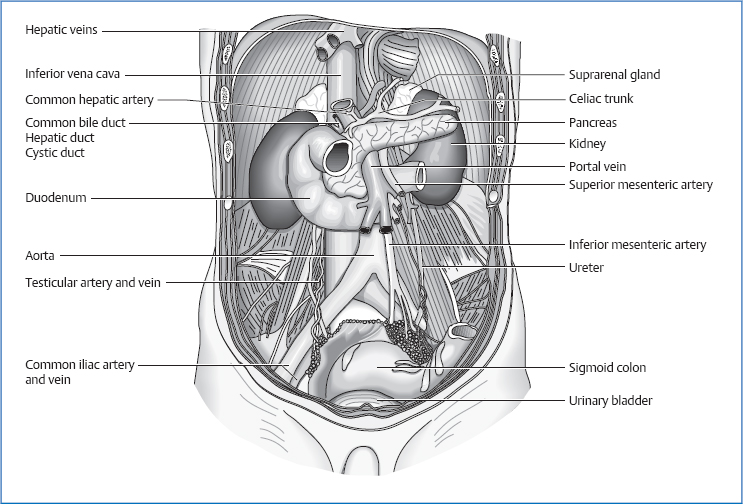
 superior mesenteric artery and vein
superior mesenteric artery and vein
 duodenojejunal flexure
duodenojejunal flexure
 omental bursa
omental bursa
 stomach
stomach
 kidneys
kidneys
 transverse mesocolon (divides the pancreas into a suband a supramesocolic part)
transverse mesocolon (divides the pancreas into a suband a supramesocolic part)
 transverse colon
transverse colon
 left colic flexure
left colic flexure
 splenic vein
splenic vein
 peritoneum
peritoneum
 spleen
spleen
 lesser omentum
lesser omentum
 portal vein
portal vein
Attachments/Suspensions
 organ pressure
organ pressure
 turgor
turgor
 attachments of connective tissue in the retroperitoneal space
attachments of connective tissue in the retroperitoneal space
 pancreaticosplenic ligament
pancreaticosplenic ligament
 retropancreatic fascia (Treitz)
retropancreatic fascia (Treitz)
 transverse mesocolon
transverse mesocolon
 duodenum
duodenum
Circulation
Arterial
 superior mesenteric artery
superior mesenteric artery
 gastroduodenal artery (from the common hepatic artery)
gastroduodenal artery (from the common hepatic artery)
 splenic artery
splenic artery
Venous
 superior mesenteric vein
superior mesenteric vein
 portal vein (from the splenic vein and pancreaticoduodenal veins)
portal vein (from the splenic vein and pancreaticoduodenal veins)
Lymph Drainage
 direct lymphatic connections to nearby organs (duodenum)
direct lymphatic connections to nearby organs (duodenum)
 via celiac lymph nodes to the gastric and hepatic lymph nodes on the left side of the body
via celiac lymph nodes to the gastric and hepatic lymph nodes on the left side of the body
 mediastinal and cervical lymph nodes
mediastinal and cervical lymph nodes
 pancreaticolienal lymph node and pylorus
pancreaticolienal lymph node and pylorus
 mesenteric and periaortal lymph nodes
mesenteric and periaortal lymph nodes
Innervation
 sympathetic nervous system from T5 to T9 (sometimes also T10 and T11) via the major splanchnic nerve, with switching in the celiac plexus
sympathetic nervous system from T5 to T9 (sometimes also T10 and T11) via the major splanchnic nerve, with switching in the celiac plexus
 vagus nerve
vagus nerve
Organ Clock
Organ-Tooth Interrelationship
Movement Physiology according to Barral
Mobility
Motility
Physiology
Insulin
 glycogen synthesis and inhibition of glycogenolysis
glycogen synthesis and inhibition of glycogenolysis
 synthesis of lipids and inhibition of lipolysis
synthesis of lipids and inhibition of lipolysis
 inhibition of protein breakdown
inhibition of protein breakdown
Glucagon
Somatostatin
 bicarbonate to neutralize the acidic chyme from the stomach
bicarbonate to neutralize the acidic chyme from the stomach
 trypsinogen and chymotrypsinogen (enzymes for digesting protein)
trypsinogen and chymotrypsinogen (enzymes for digesting protein)
 α-amylase (also present in the saliva of the mouth) for cleaving carbohydrates
α-amylase (also present in the saliva of the mouth) for cleaving carbohydrates
 lipase (enzyme for cleaving fat)
lipase (enzyme for cleaving fat)
Pathologies
Symptoms that Require Medical Clarification
Acute Pancreatitis
Causes
 biliary tract disorders (40–50%)
biliary tract disorders (40–50%)
 alcohol abuse (30–40%)
alcohol abuse (30–40%)
 idiopathic (10–30%)
idiopathic (10–30%)
 medications (diuretics, β blockers, glucocorticoids, antibiotics, nonsteroidal antirheumatics)
medications (diuretics, β blockers, glucocorticoids, antibiotics, nonsteroidal antirheumatics)
 trauma
trauma
 infections (mumps, Coxsackievirus)
infections (mumps, Coxsackievirus)
 hypercalcemia (e.g., hyperparathyroidism)
hypercalcemia (e.g., hyperparathyroidism)
 hyperlipoproteinemia
hyperlipoproteinemia
 papillary stenosis
papillary stenosis
Clinical
 guiding symptom: severe upper abdominal pain, arising approximately 8–12 hours after a large meal or alcohol abuse, with pain radiating into the back and ringlike to the left around the torso
guiding symptom: severe upper abdominal pain, arising approximately 8–12 hours after a large meal or alcohol abuse, with pain radiating into the back and ringlike to the left around the torso
 shock
shock
Chronic Pancreatitis
Causes
 alcohol (70–90%)
alcohol (70–90%)
 idiopathic (10–25 %)
idiopathic (10–25 %)
 anomalies in the pancreatic duct system
anomalies in the pancreatic duct system
 hyperparathyroidism
hyperparathyroidism
 trauma
trauma
 abuse of analgesics
abuse of analgesics
Clinical
 upper abdominal pain
upper abdominal pain
 nausea, vomiting
nausea, vomiting
 icterus
icterus
 depression
depression
 diabetes mellitus
diabetes mellitus
 constipation
constipation
 thrombophlebitis
thrombophlebitis
 excretory insufficiency
excretory insufficiency
 weight loss
weight loss
 steatorrhea
steatorrhea
 diarrhea
diarrhea
 meteorism
meteorism
 edemas
edemas
Pancreatic Cancer
 weight loss
weight loss
 recurrent thrombophlebitis
recurrent thrombophlebitis
 back pain
back pain
 obstructive icterus
obstructive icterus
Osteopathic Practice
Cardinal Symptoms

Related posts:


Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


