Chapter 11 The Knee
The knee is the largest joint in the body. The lower portion of the femur and upper aspect of the tibia articulate at only two points where the rounded femoral condyles bear weight on the flat tibial plateaus. The knee joint is subject to a wide variety of traumatic, mechanical, and inflammatory disorders.
Anatomy
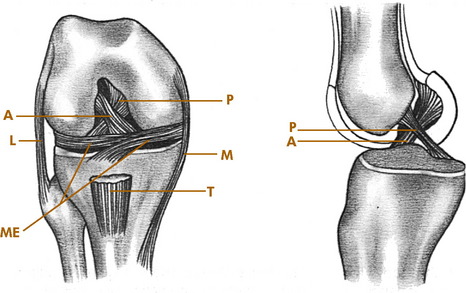
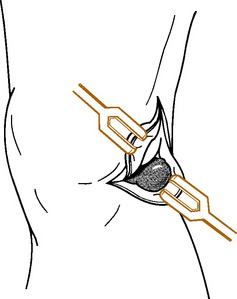
The knee joint consists of medial and lateral, femoral and tibial condyles; and the patella. It is essentially a round bone sitting on a flat bone with no intrinsic bony stability and depends completely on its ligaments, muscles, menisci, and capsule for support. The most important ligaments of the knee are the medial and lateral collateral ligaments (LCLs) along with their associated posterior capsular structures and the anterior and posterior cruciate ligaments (Fig. 11-1). The medial collateral ligament originates below the adductor tubercle and attaches to the upper medial tibia. It limits abduction and assists in controlling rotation. The LCL attaches to the lateral epicondyle of the femur and head of the fibula and controls adduction. The cruciate ligaments attach to the intraarticular portions of the femur and tibia. The anterior cruciate ligament (ACL) prevents anterior displacement of the tibia and helps control rotation of the tibia on the femur. The posterior cruciate ligament (PCL) prevents backward displacement of the tibia on the femur.
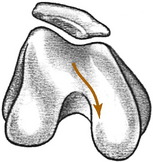
Normal knee motion consists of a combination of rotation and either extension or flexion. Normally, as the knee flexes, the tibia internally rotates. Extension of the knee is accompanied by lateral or external rotation of the tibia. These rotational motions are controlled by the ligaments and menisci of the knee. This rotation is reflected in the course that the patella takes with flexion and extension movements (Fig. 11-2). Thus, damage to the knee (such as a torn meniscus, which prevents normal tibial rotation) can cause patellar symptoms resulting from abnormal patellar excursion. These patellar symptoms are typically aggravated by walking up and down stairs, an activity that puts the greatest strain on the patella and knee extensors.
Roentgenographic Anatomy
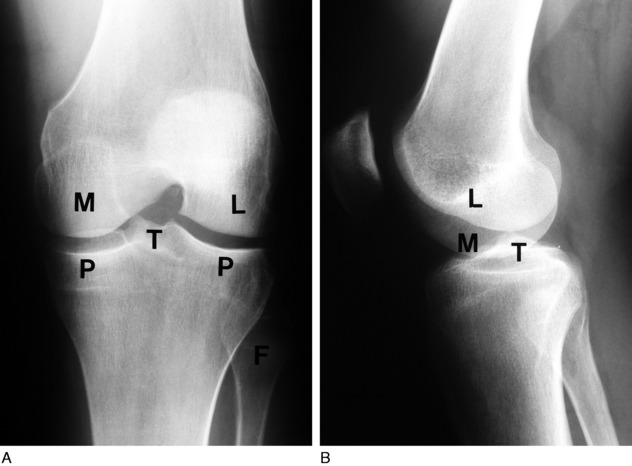
Anteroposterior and lateral views are essential in the diagnosis of knee disorders (Fig. 11-3). A tunnel view visualizes the intercondylar notch, and tangential views are helpful in diagnosing patellar disorders. With patients over the age of 40, the anteroposterior view should always be performed with the patient standing. This may reveal subtle joint space narrowing if osteoarthritis is present.
Lesions of the Meniscus
INJURIES OF THE MENISCUS
The menisci, or semilunar cartilages, are two C-shaped structures composed of fibrocartilage that help act as cushions between the femur and tibia. They also assist in the control of normal knee motion. If the normal rotation of the tibia is forcibly prevented as the knee is flexed or extended (that is, if flexion occurs with external rotation or extension occurs with internal rotation), a tear in the meniscus can occur. The injury may be isolated or in conjunction with ligamentous ruptures. Meniscus tears are the most common of all knee injuries, and the pathologic characteristics of the tear are variable (Fig. 11-4). When an injury occurs that produces free fragments or tears, healing to the main body of the meniscus may not take place. The fragment often remains permanently detached but viable because nourishment for the meniscus is provided by the joint fluid. This joint fluid circulates around the tear and often prevents healing from taking place. Persistent symptoms are the result. The medial meniscus is injured 10 times more frequently because it is more firmly attached and less mobile than the lateral meniscus. In long-standing disease, articular cartilage erosion of the tibiofemoral and patellofemoral joints may even result.
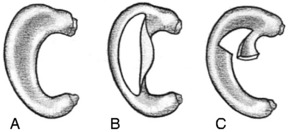
FIG. 11-4 A, Normal meniscus. B, Longitudinal, or “bucket-handle,” tear. C, Tear of the posterior horn.
CLINICAL FEATURES
The examination usually reveals a joint effusion (Fig. 11-5). Its presence indicates acute or chronic synovial irritation. Its absence by history or examination should cause another diagnosis to be considered. This fluid may cause the patella to be ballotable. A click may also be present when the patella is pressed against the femur.

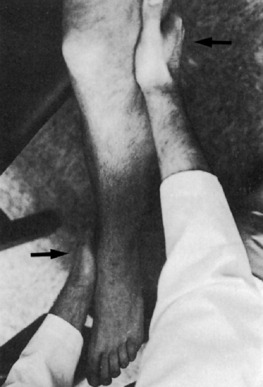
Pain and tenderness at the joint line either medially or laterally may be present. The range of motion is frequently limited. This may be caused by swelling, pseudolocking, or occasionally the interposition of the torn meniscus. In long-standing disease, atrophy of the quadriceps muscle, especially the vastus medialis, occurs rapidly (Fig. 11-6).

The McMurray test is sometimes helpful in detecting a meniscus tear, although it is difficult to perform on a painful, swollen knee, and the results are often inconsistent (Fig. 11-7). Full knee flexion, which increases pressure on the posterior horns, may cause pain with many meniscus tears.
SPECIAL STUDIES
TREATMENT
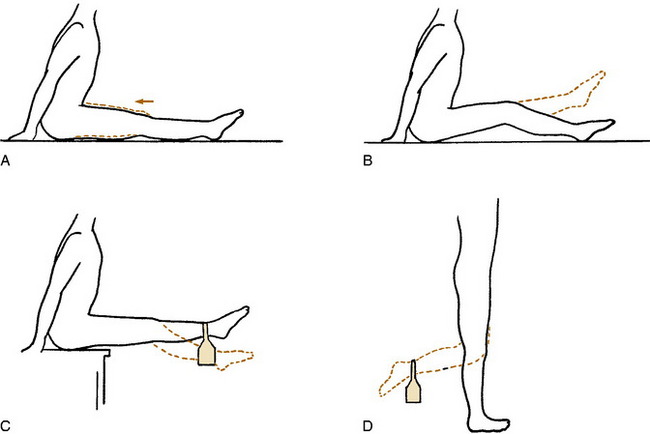
The initial treatment is conservative, except for those rare cases in which the knee is truly locked. Many meniscus tears, especially peripheral ones, can heal spontaneously in a few weeks. A bulky compression dressing (often called the “Robert Jones” dressing) and ice are applied if the injury is acute, and the knee is elevated (Fig. 11-8). The patient is placed on crutches and started on quadriceps-strengthening exercises (Fig. 11-9). These exercises will help compress out the joint effusion and maintain strength, and they should always be performed with the knee near complete extension to prevent patellofemoral pain from developing. Gentle range-of-motion exercises are started in 2 to 3 days. Swimming is an excellent exercise for increasing motion and decreasing discomfort. As pain subsides and motion returns, weight-bearing activities are gradually resumed, but quadriceps exercises are continued for 2 to 4 weeks. There are few indications for aspiration of the knee and even fewer indications for the injection of steroids in the treatment of an acute injury. The protective responses of the patient should be maintained, and it is better to reduce swelling by quadriceps contractions and to rehabilitate the knee through exercises.

Comments
Meniscal “tears” are common in conjunction with osteoarthritis of the knee, and if the two disorders occur together, which they often do, it is virtually impossible to determine whether the meniscal abnormality is the source of pain. This calls into question the usefulness of MRI (and meniscal surgery) in the older patient who already has degenerative disease on plain films. The likelihood of finding a meniscal tear in the presence of moderate osteoarthritis is almost 90%, and MRI probably adds very little to the decision-making process in these patients. Decisions regarding the usefulness of meniscectomy in these patients should be made on a clinical basis (mechanical symptoms, joint line tenderness, and so on), but even these features lack specificity in this group of patients.
CALCIFICATION OF THE MENISCI
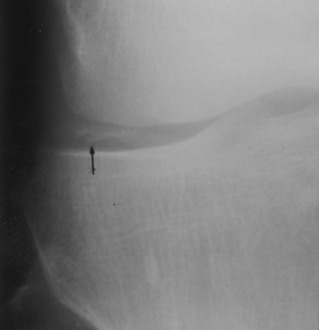
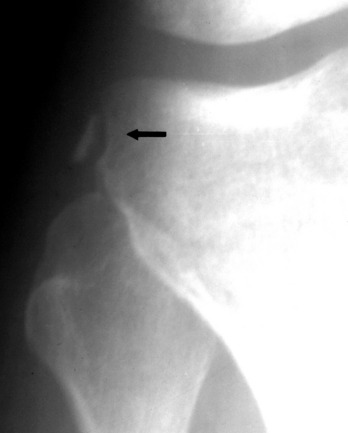
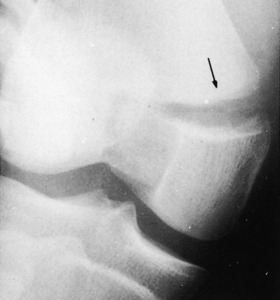
The meniscus can become calcified from a variety of causes (Fig. 11-10), the most common being degeneration and trauma. However, calcification can also occur in several other conditions, including degenerative arthritis, ochronosis, and pseudogout. The calcification itself is usually not painful. The symptoms are those that result from the primary disorder, and treatment is directed at that disorder.
Cysts
CLINICAL FEATURES
In children, the symptoms are usually related to the effects of direct pressure of the cyst on the adjacent soft tissues. Local discomfort may be present. In adults, the symptoms are related not only to the effects of the pressure of the cyst but also to the primary intraarticular abnormality. (Many cysts are asymptomatic, however.) The cyst commonly changes in size, depending on the activity of the patient and the amount of swelling in the knee.
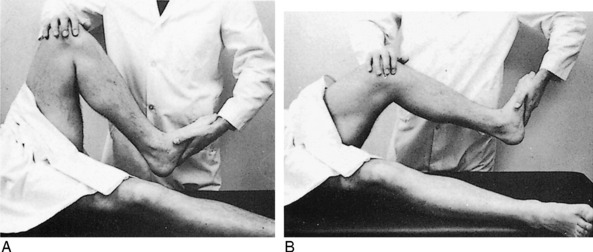
Examination will reveal a cystic mass of variable size lateral to the medial hamstrings in the popliteal fossa (Fig. 11-11). The lesion may be locally tender. Other findings of primary joint disease may be present, especially in adults.

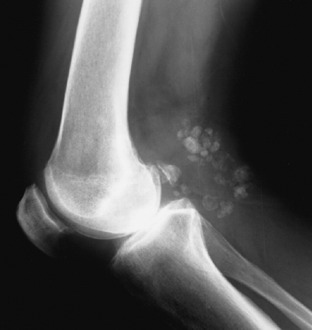
Except for occasional osteoarthritis, the roentgenogram is usually normal. Ultrasound studies are easy and can document the cystic nature of the lesion when the diagnosis is in doubt. They are also cost effective. MRI can identify underlying joint pathology as well. Occasionally, the cyst may even form multiple calcific loose bodies (Fig. 11-12).
TREATMENT
Adult patients are primarily treated nonsurgically. The cyst may be aspirated to reassure the patient of its benign nature. Aspiration, sometimes with injection of 1 mL of steroid, is often performed to relieve symptoms, and although recurrence is common, the symptoms are usually more tolerable. An intraarticular injection may also be needed to suppress the synovitis. If surgery is being considered, every attempt should be made to detect any underlying joint abnormality. Cyst excision without correction of the intraarticular abnormality is followed by a high rate of recurrence of the cyst. Correction of the intraarticular condition also frequently renders cyst excision unnecessary because the cyst becomes asymptomatic following elimination of the cause of the chronic effusion. Most patients are treated successfully by aspiration alone, or simple observation if the cyst is not symptomatic.
CYSTS OF THE MENISCUS
Cysts may also develop in a meniscus, usually the lateral, as a result of degeneration or trauma. The patient is generally a young adult who has a history of pain and a gradually enlarging mass over the lateral joint line (Fig. 11-13). A knee effusion may be present. Treatment consists of aspiration or meniscectomy and cyst excision if the patient is symptomatic.
Lesions of the Ligaments
CLINICAL FEATURES


TREATMENT
Treatment of cruciate injuries varies, depending on the age and activity of the patient and the presence of any additional injuries. Isolated ACL and PCL ruptures are generally treated nonsurgically, at least initially, in many cases. Reconstruction is usually required in patients with high demands. A well-constructed brace may provide an option in some patients. The treatment of combined cruciate/collateral injuries is unsettled. Surgery may be required to improve joint stability in the patient with multiple ligament involvement.
Minor ligament sprains are treated in the same manner as meniscus injuries (Fig. 11-19). Immobilization in a compression dressing with ice and elevation for 2 to 3 days are followed by exercises to promote absorption of swelling and restoration of motion and strength.
CHRONIC INSTABILITY
Patients often present with episodes of the knee “giving way” or “going out,” especially with activities that require cutting or changing directions. A chronic effusion may be present in the knee. Although a torn meniscus can cause similar symptoms, the most common cause of this problem is chronic instability caused by ACL deficiency. Although the initial disability from isolated ACL injuries may seem minimal, the injury may result in progressive deterioration with increasing knee laxity, tears in either meniscus, and articular cartilage degeneration. The ACL rupture has been referred to as “the beginning of the end” of the athlete’s knee.
Older injuries often cause the knee to “give out,” a term usually called the pivot shift.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


