Chapter 19 The Ida Rolf Method of Structural Integration
 Initial Examination
Initial Examination
Recreational Activities: Swimming
General Health: Good; she is pre-menses
Neuromuscular: Force generation: Left knee and hip extension 3+/5 and right are 4/5; rectus abdominis and obliques are 2/5. Upper extremity strength is within functional limits. Resistance to passive movement of adductors and internal rotators is 1+ on Ashworth Scale.1,2 Pain Visual Analogue Scale (VAS) is a 4 to 5/10 for her lower back at the end of the day, especially after prolonged walking.
Function: Ambulates in school pain free until third period, when symptoms begin. Timed up and go (TUG)3 used to measure ambulation speed on 10-meter walk test was 10.9 seconds. She required 25 seconds to ascend and descend one flight of nine steps. Independent with activities of daily living (ADL), except donning and doffing shoes requires minimum assistance. On the Gross Motor Function Classification Scheme (GMFCS) she is a Level II.4
 Evaluation and Plan of Care
Evaluation and Plan of Care
Susan presents with musculoskeletal, cardiopulmonary, and neuromuscular impairments that may be causing her low back symptoms and limited ambulation. Her physical therapy program is designed to reverse some of those impairments and provide task-specific training to improve functional mobility. The plan includes prolonged stretching of erector spinae, quadratus lumborum, and lower extremity tight muscles, lower extremity and abdominal strengthening using endurance training on a bicycle, and incentive spirometry. Ambulation speed and distance at school will be monitored and timed by wearing a pedometer. Stretching and strengthening program to be executed daily with assistance of parent and reevaluation in 2 weeks.
 Reevaluation
ReevaluationINVESTIGATING THE LITERATURE
Preliminary Reading
The therapist collaborates with a clinician scientist who is familiar with SI because she has performed some research in the area. The preliminary reading provided to the therapist by the scientist consists of writings by Ida Rolf, who is the originator of the approach. Rolf’s theoretical framework and concepts supporting the method first were described in an article5 and then elaborated on in her book, Rolfing: The Integration of Human Structures.6 Additional information about the approach can be gained from a book in which Rolf is interviewed about Rolfing.7 Other useful sources are brief descriptions of the approach found on the websites of the two main organization that train practitioners, the Guild for Structural Integration and the Rolfing Institute8,9; a three-part series on SI published by a Rolfing practitioner in the Journal of Body Work Movement Therapies10–12; and chapters written in bodywork13 and complementary therapy books.14,15
SI is a systematic approach of tissue-based work and elements of movement reeducation designed to improve the alignment and function of the body. Two main organizing principles of the approach are the interaction of the body with gravity and the role of the fascia as a central organ of the body. Rolf believed that the body’s alignment was organized with respect to gravity. Through use, disuse, and even abuse optimal alignment is compromised, which leads to pain and movement difficulties. She believed that this process could be reversed by the use of manual techniques to remodel the fascia, which supports all of the tissues in the body.
The 10 sessions of SI are sometimes referred to as a recipe.7 This statement is accurate, to some extent, because a systematic approach to each examination and intervention is used. The general examination consists of a three-dimensional examination of posture. This is done by observing posture using Rolf’s stacked blocks model of the body (Figure 19-1). Alignment of the blocks in three planes is the standard for optimal posture. The pelvis is considered the central block. The second element of the evaluation is observation of tissue appearance. Evidence of pulling and tightness is an indicator of restriction or tonal changes in the tissue. Observation of bony and soft tissue structures also takes place during movement. The SI metaphor used to describe tissue movement is “the sleeve and core.” The sleeve corresponds to appendicular structures that are to move freely over the core or axial structures.
Figure 19-1 Rolfing postural view.
(From Rolf IP: Rolfing: the integration of human structures, New York, 1997, Harper & Row, p 33.)
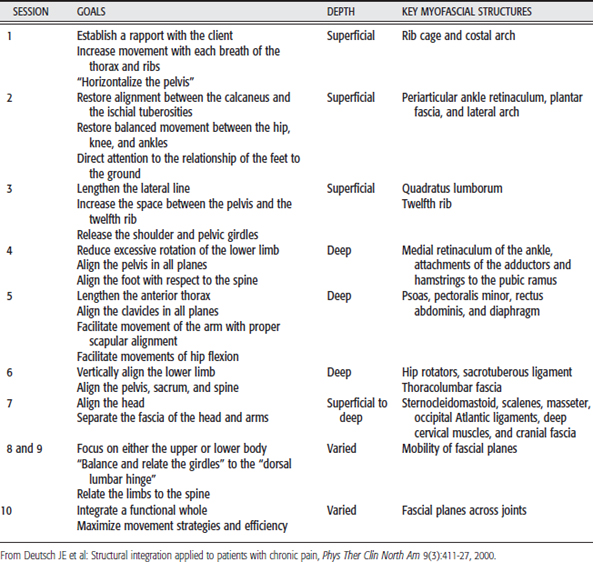
Each session has a specific intent; therefore the examination and intervention are adjusted further to focus on a set of soft tissue structures and appropriate movement cues. Specific movements are selected because they relate to the goals of a session. For example, in the first session breathing is observed to begin work on the anterior chest. Identification of deviations in posture and tissue restrictions related to breathing help locate dysfunction and guide practitioners’ interventions. The intent of each examination and primary structures addressed for each session are summarized in Table 19-1.
The intervention consists of soft tissue mobilization by application of the amount of pressure required to free restrictions. The goal is to remove any fascial adherences that prevent structures from being in their optimal alignment. For example, during the second session practitioners focus on the alignment of the lower extremities and work primarily on the superficial soft tissue of the feet and leg, such as the retinaculum on the dorsum of the foot; the perimalleolar structures, such as the peroneal tendons; the gastrocnemius muscles; the medial and lateral collateral ligaments; the tibial crest; the Achilles tendon to the calcaneus; and the medial and lateral arch.15
The focus of each session, in addition to the depth of the soft tissue work, is varied systematically. Sessions one through six alternate their emphasis on either the upper (odd numbered, 1, 3, and 5) or lower (even numbered, 2, 4, and 6) part of the body. The depth of the work begins superficially in the first session, working on the fascia of the sternocleidomastoid in the neck, and moves to the deepest structures in the fourth session, such as the insertion of the adductors on the pubic ramus. In sessions seven through 10, the work is done on large fascial planes that connect the upper and lower part of the body. The main structures addressed and the depth of the work are summarized in Table 19-1. A more detailed description of the first six sessions can be found in the Guild News16,17 and a description of the entire series can be found in the Journal of Body Work Movement Therapies.10,11,12
In addition to alignment with respect to gravity and the fascial organization of the body, the role of the parasympathetic nervous system appears to be important in SI. One of the manual techniques used in each session is a pelvic lift. It is performed with the client supine and the knees flexed. One hand is placed on the sacrum, with the fingertips resting on the lumbosacral junction. The second hand is placed on the subject’s epigastrum to stabilize the trunk. A cranial traction force is applied, using the hand on the lumbosacral junction to rotate the pelvis posteriorly.18 Evidence suggests that use of this pelvic lift increases parasympathetic tone and therefore is associated with a relaxation response.18,19
Biomechanical alignment with respect to gravity and manipulation of the autonomic nervous system are two of the mechanistic explanations of SI. A third explanation proposed by Oschman is energetic.20 He described the tissue as having semiconductor properties that could be altered by the soft tissue work. Oschman describes Rolf’s work as benefiting from the plasticity of connective tissue.
Sessions typically are performed in 1-week intervals. This is done to allow the body to reorganize itself with respect to gravity. After the 10-session process is completed, individuals may be reevaluated if their symptoms persist. This is more likely to be the case if the person returns to habitual movement patterns and postures that created the original myofascial imbalance. Additional lessons are offered with a greater emphasis on movement reeducation or as tune-up sessions.21

Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


