Chapter 10. The hip
SUMMARY
Pain in the hip region can be incorrectly attributed to the lumbar spine and/or sacroiliac joint, while the bursae in the area may not be considered, and can evade diagnosis. Groin strain and hamstring injury are familiar to the clinician, though worthy of mention to enhance effective treatment.
This chapter describes the anatomy relevant to common lesions in the hip region to which orthopaedic medicine principles of treatment can be applied. A commentary follows, highlighting the relevant points of the history and suggesting a methodical sequence for objective examination. Lesions are then discussed with treatment alternatives and overall management.
ANATOMY
Inert structures
The hip joint is a synovial joint formed between the head of the femur and the acetabulum of the innominate bone. The head of the femur is slightly more than half a sphere and faces anteriorly, superiorly and medially to articulate with the acetabulum forming a ball-and-socket joint. This articulation offers great stability and provides sufficient mobility for gait. The close packed position of the hip joint is full extension, with a degree of abduction and medial rotation (Hartley 1995, Standring 2009).
The acetabulum is deepened by the fibrocartilaginous acetabular labrum and all articular surfaces are covered by articular cartilage. The fibrous capsule, lined with synovium, surrounds most of the neck of the femur, attaching above to the acetabular rim, below to the intertrochanteric line anteriorly and 1 cm above the inter-trochanteric crest posteriorly. Both the joint capsule and the articular cartilage tend to be thicker anterosuperiorly, which is the region of most stress in weight-bearing. Synovial plicae (folds or reflections of the synovial membrane) have been identified by Fu et al (1997), found mainly on the external surface of the lower medial part of the acetabular labrum (labral plicae) but also at the base of the ligament of the head of the femur and on the base of the femoral neck. The labral plicae may potentially be a source of pain if injured or thickened since, in the normal state, these have been seen to slip between the articular surfaces of the femoral head and acetabulum during medial rotation and to return to their original position during lateral rotation.
Three ligaments reinforce the articular capsule and control movement. All three are taut in extension and relaxed in flexion. The iliofemoral ligament has strong medial and lateral bands which form a Y-shape, passing from the anterior inferior iliac spine to the intertrochanteric line. The pubofemoral ligament passes from the superior pubic ramus to blend distally with the capsule and the medial border of the iliofemoral ligament. The ischiofemoral ligament passes from the ischium and winds superiorly and laterally to the upper part of the femoral neck, blending with the capsule of the hip joint and supporting it posteriorly.
The psoas bursa (L2–L3; Cyriax 1982) is 5–7 cm long and 2–4 cm wide in its normal collapsed state (Underwood et al 1988, Toohey et al 1990, Flanagan et al 1995, Zimmermann et al 1995). In 15% of cadaveric specimens, the psoas bursa was seen to communicate with the hip joint via an aperture between the iliofemoral and pubofemoral ligaments (Flanagan et al 1995). It may be a simple bursa or multiloculated with well-defined thin walls (Meaney et al 1992).
The psoas bursa lies beneath the musculotendinous junction of the iliopsoas muscle and the front of the capsule of the hip joint (Fig. 10.1). It cushions the ilio-psoas tendon as it winds round the front of the hip joint to its posteromedial insertion on the lesser trochanter. It is related anteromedially to the femoral artery and anteriorly to the femoral nerve (Canoso 1981). Its point of location is just distal to the midpoint of the inguinal ligament, deep to the femoral artery.
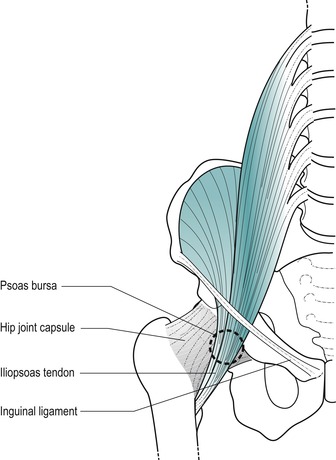 |
| Figure 10.1 Position of the psoas bursa. |
The gluteal bursa (L4–L5; Cyriax & Cyriax 1993) is not a single entity, but for clinical purposes is considered to be so. At least four separate bursae lie between the different planes of the gluteal muscles as they attach to or pass over the greater trochanter, collectively forming the gluteal bursa.
Two bursae are associated with gluteus maximus: a large trochanteric bursa (Fig. 10.2), separating it from the lateral aspect of the greater trochanter, and a gluteofemoral bursa, lying between it and vastus lateralis (Standring 2009). The trochanteric bursa of gluteus medius lies between its tendon and the anterosuperior aspect of the greater trochanter. The trochanteric bursa of gluteus minimus separates its insertion from the medial part of the greater trochanter (Standring 2009). One further bursa may be present, the ischial bursa, lying between the ischial tuberosity and the lower part of gluteus maximus.
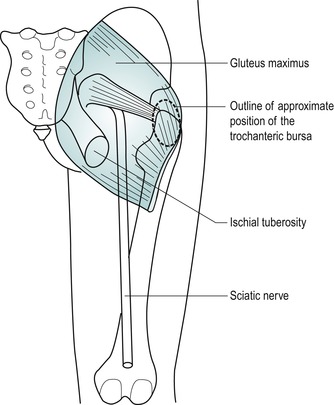 |
| Figure 10.2 Position of trochanteric bursa. |
Contractile structures
Anterior muscles are flexors of the hip, although they may also assist other hip movements. Some pass over the knee where they also have an effect. Resisted flexion of the hip tests mainly psoas major; with the knee flexed it is also testing rectus femoris.
Psoas major (ventral rami L1–L3) has its origin from the lumbar spine. It descends to pass under the centre of the inguinal ligament receiving the fibres of iliacus on its lateral side. The iliopsoas tendon crosses the front of the hip joint where it is cushioned by the underlying psoas bursa. The combined tendon winds posteriorly to insert into the lesser trochanter of the femur.
Sartorius (femoral nerve L2–L3) passes from the anterior superior iliac spine to cross the thigh medially, inserting into the upper medial aspect of the tibia. It marks the lateral border of the femoral triangle.
Rectus femoris (femoral nerve L2–L4) is part of the quadriceps mechanism and has its main effect at the knee. However, its origin above the hip makes it a two-joint muscle and it also acts as a powerful hip flexor, being most efficient when the knee is flexed (Kapandji 1987). It has two heads of origin: a straight head from the anterior inferior iliac spine and a reflected head from just above the acetabular rim. It joins the rest of the quadriceps to insert into the patellar tendon.
Posterior muscles are extensors of the hip. Gluteus maximus acts principally as a hip extensor while the hamstrings assist hip extension, but their main effect is in flexing the knee. Since the hamstring muscles run over two joints, their efficiency in extending the hip increases if the knee is locked into extension (Kapandji 1987).
Gluteus maximus (inferior gluteal nerve L5, S1–S2) is the largest and most superficial of the gluteal muscles. It passes from behind the posterior gluteal line on the blade of the ilium to the iliotibial tract and upper femur. The large trochanteric bursa separates the insertion of gluteus maximus from the lateral aspect of the greater trochanter.
Biceps femoris (sciatic nerve L5, S1–S2) is the lateral hamstring with two heads of origin. A long head arises from an inferomedial facet on the ischial tuberosity (which it shares with semitendinosus) and a short head from the lateral lip of the linea aspera. Its fibres converge into a fusiform muscle belly and its tendon of insertion attaches to the head of the fibula.
Semitendinosus and semimembranosus are the medial hamstrings. Semitendinosus (sciatic nerve L5, S1–S2) takes origin from the inferomedial facet on the ischial tuberosity. Its muscle belly ends in the middle of the thigh and its long tendon of insertion lies on semimembranosus before winding around to the medial aspect of the upper tibia. Semimembranosus (sciatic nerve L5, S1–S2) takes origin from the superolateral facet on the ischial tuberosity and has its main insertion onto the posterior aspect of the medial tibial condyle into the tuberculum tendinis.
Functionally, the small, deep muscles of the hip are responsible for lateral rotation.
Piriformis (L5, S1–S2) originates in the pelvis, exiting through the greater sciatic foramen to attach to the upper border of the greater trochanter.
Obturator externus (posterior branch of the obturator nerve L3–L4) and obturator internus (nerve to obturator internus L5, S1) pass posteriorly to the hip joint and insert into the medial surface of the greater trochanter and trochanteric fossa.
Gemelli (L5, S1) pass from the ischial spine and ischial tuberosity to the medial aspect of the greater trochanter.
Quadratus femoris (nerve to quadratus femoris L5, S1) passes from the ischial tuberosity to the quadrate tubercle in the middle of the trochanteric crest.
Lateral muscles are abductors and lateral rotators. Gluteus medius is the main hip abductor while medius and minimus together are responsible for maintaining the position of the opposite side of the pelvis in single-leg stance. Weakness of the hip abductors produces a positive Trendelenburg sign. Tensor fascia lata and the anterior fibres of gluteus medius and minimus also produce medial rotation and flexion because they lie anterior to the frontal plane of the hip joint. Lying posteriorly, some fibres of gluteus medius and minimus are responsible for lateral rotation and extension (Kapandji 1987).
Gluteus medius (superior gluteal nerve L5, S1) is partially overlapped by maximus and lies in a slightly deeper plane. It originates from the blade of the ilium between posterior and anterior gluteal lines and inserts into the lateral aspect of the greater trochanter.
Gluteus minimus (superior gluteal nerve L5, S1) is the deepest gluteal muscle and arises between the anterior and inferior gluteal lines, inserting into the medial part of the anterior trochanteric surface.
Tensor fascia lata (superior gluteal nerve L4–L5) arises from the anterior 5 cm of the outer lip of the iliac crest and the anterior superior iliac spine. It passes downwards and laterally to insert into the anterior border of the ilio-tibial tract.
The adductor muscles originate in the pelvis and pass to the medial aspect of the thigh.
Functionally, the medial muscles are responsible for adduction of the hip. Medial rotation at the hip is a secondary function of gluteus medius, minimus and tensor fascia lata; adductor magnus, longus and pectineus may also contribute to this movement.
Gracilis (obturator nerve L2–L3) is the most medial hip adductor. It passes from the lower half of the body of the pubis, the inferior pubic ramus and the adjacent ischial ramus, to run vertically downwards to just below the medial tibial condyle.
Pectineus (femoral nerve L2–L3) passes from the pecten pubis running posterolaterally to a line joining the lesser trochanter to the linea aspera.
Adductor longus (obturator nerve L2–L4) is the most superficial adductor. It passes from the body of the pubis, in the angle between the crest and the symphysis pubis, to descend posterolaterally to the middle third of the linea aspera.
Adductor brevis (obturator nerve L3) lies deep to adductor longus, passing from the lower aspect of the body of the pubis and the inferior pubic ramus to its attachment on the femur, between the lesser trochanter and the linea aspera.
Adductor magnus (upper fibres, obturator nerve; lower fibres, tibial branch of the sciatic nerve, L2–L4) is the largest and deepest adductor muscle. It is considered to have two separate portions, one an adductor portion and the other a hamstring portion, each with its own separate nerve supply. It takes origin from the inferior pubic ramus, the adjacent ischial ramus and the infero-lateral aspect of the ischial tuberosity. Its upper fibres pass mainly horizontally to the linea aspera of the femur and form the adductor part of the muscle. Its lower fibres pass more vertically to the adductor tubercle on the medial femoral condyle and form the hamstring part.
A GUIDE TO SURFACE MARKING AND PALPATION
Pelvis region
Palpate the iliac crest, which should be obvious in most people as no muscles attach to its superior border. The highest point of the crest lies just posterior to the midpoint and gives an approximate indication of the level of the spinous process of L4.
Palpate the anterior superior iliac spine which is sub-cutaneous and located at the anterior end of the iliac crest. It marks the lateral attachment of the inguinal ligament and the origin of the sartorius muscle.
Palpate the posterior superior iliac spine which is situated at the posterior end of the iliac crest. It is not as readily palpable as the anterior spine, but lies under a dimple in the upper buttock, approximately 4 cm lateral to the spinous process of S2. It gives attachment to the sacro-tuberous ligament. Imagine a line drawn from the posterior superior iliac spine to the spinous process of S2; this line crosses the centre of the sacroiliac joint and gives an indication of the joint’s position.
Consider the position of the anterior and posterior inferior iliac spines which lie below the superior spines and are not as readily palpable. The anterior inferior spine gives origin superiorly to the long head of rectus femoris and inferiorly to part of the iliofemoral ligament.
Locate the position of the pubic tubercle at the medial end of the inguinal crease, lying at the same level as the top of the greater trochanter. It marks the medial attachment of the inguinal ligament.
Palpate the bony ischial tuberosity, which lies in the buttock approximately 5 cm lateral to the midline just above the gluteal fold. In the sitting position, body weight is supported by the ischial tuberosities. Each is most easily palpated with the patient in side-lying and the hip placed in flexion, to bring the ischial tuberosity out from under the bulk of gluteus maximus.
Lateral aspect of the thigh
In side-lying palpate the greater trochanter, which is a large quadrangular bony prominence situated at the upper lateral shaft of the femur, approximately one hand’s breadth below the iliac crest. Grasp the greater trochanter with your thumb, index and middle fingers (Fig. 10.3), lifting the leg passively into abduction to relax the iliotibial tract. The greater trochanter will be a useful bony landmark for some of the injection techniques around the hip.
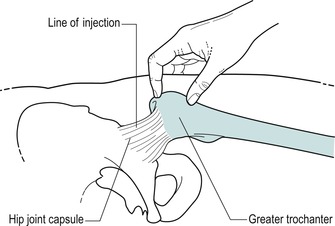 |
| Figure 10.3 Location of hip joint for the injection by grasping the greater trochanter. |
Anterior aspect of the thigh
Consider the position of the femoral triangle on the anterior thigh (Fig. 10.4). Place the leg into the FABER position – a combination of Flexion, ABduction and External (lateral) Rotation of the hip – to give you an indication of the borders of the triangle. The inguinal ligament forms the base of the triangle, sartorius its lateral border and adductor longus its medial border. Iliopsoas and pectineus lie in the floor of the femoral triangle.
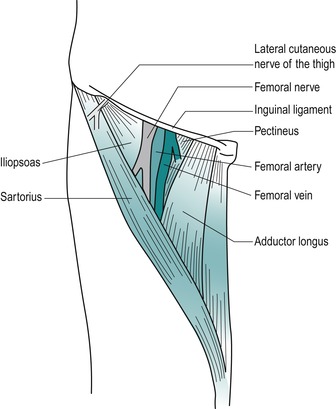 |
| Figure 10.4 Femoral triangle, also showing emerging lateral cutaneous nerve of thigh. |
Consider the position of the lateral femoral cutaneous nerve of the thigh (L2–L3) as it passes under or through the inguinal ligament, just medial to the anterior superior iliac spine. It may be compressed here, causing a condition called meralgia paraesthetica, which produces paraesthesia and pain in the nerve’s distribution on the lateral side of the thigh. It is found in obese patients and those who wear tight-fitting clothes or belts (Adkins & Figler 2000).
Palpate for the femoral artery which passes down through the middle of the triangle with the femoral vein situated medially and the femoral nerve laterally. You will locate a strong pulse just distal to the midpoint of the inguinal ligament.
Locating the femoral pulse will prove a useful landmark for the structures passing deep to it. From superficial to deep these are the iliopsoas tendon, which is en route to its insertion into the lesser trochanter, the psoas bursa, and the hip joint.
Posterior aspect of buttock and thigh
Consider the position of the sciatic nerve in the buttock (Fig. 10.5). You can locate its approximate position by marking a point midway between the posterior superior iliac spine and the greater trochanter, which identifies the position of the nerve as it leaves the pelvis via the greater sciatic foramen, emerging under piriformis. Join this to another mark at a point just medial to the midpoint between the greater trochanter and the ischial tuberosity. This indicates the position of the nerve as it continues to exit the buttock under the lower border of gluteus maximus (Standring 2009).
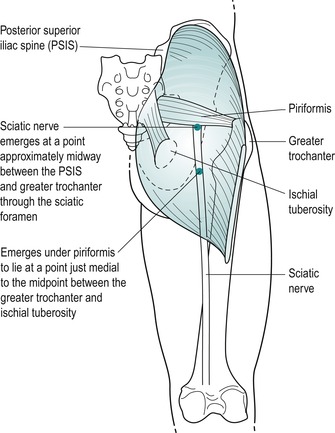 |
| Figure 10.5 Approximate course of the sciatic nerve in the buttock and thigh. |
COMMENTARY ON THE EXAMINATION
Observation
A general observation is made of the patient’s face and overall posture, but particular attention is paid to the gait. Since the function of the hip joint is to support body weight, lesions involving the joint mechanics tend to cause alterations in the gait pattern. An uneven stride will indicate restricted movement, as found in arthritis, or may be due to pain on weight-bearing. Excessive lateral rotation on walking may indicate a slipped epiphysis in the young or may be present with pain or advanced capsular contracture in the elderly, indicating an arthrosis with a marked capsular pattern. A Trendelenburg gait will indicate weak abductor muscles.
Pain in the hip joint region may originate in the lumbar spine and a detailed history will help to eliminate a lesion in the area.
History (subjective examination)
The age, occupation, sports, hobbies and lifestyle of the patient may alert the examiner to the possible cause of the lesion.
The age of the patient is relevant to conditions at the hip. Degenerative osteoarthrosis typically presents in the middle to older age group, although it is not uncommon to find it in younger athletes, especially road runners. Muscle lesions and bursitis affect the middle age group, while loose bodies can present as a complication of osteo-arthrosis in the older group or as osteochondritis dissecans in adolescents.
Children can develop hip problems which if misdiagnosed can be potentially serious, and an orthopaedic opinion should always be sought. ‘Irritable hip’ is a non-specific diagnosis for groin pain, limited movement and a limp. Perthes’ disease affects boys aged 3–10 and is an osteochondritis of the femoral epiphysis. Slipped epiphysis is either sudden or gradual slipping of the superior epiphyseal plate which may produce a lateral rotation deformity. It tends to occur in overweight adolescents (10–16) and is more common in boys, who present with pain on exercise. Transient synovitis is of unknown aetiology and affects children under 10 years with an acute onset (Gough-Palmer & McHugh 2007). Juvenile chronic arthritis usually begins in other joints, but it can also affect the hip joints. Emms et al (2002) remind us that, although it is well known that knee pain in children may be referred from the hip, it must not be forgotten that hip pathology may masquerade as knee pain in adult patients as well.
Excessive muscle contraction, as involved in explosive sports changing rapidly from running to jumping (hurdling, etc.), can lead to avulsion fractures and chronic apophysitis in adolescents, most commonly at the origin of the long head of rectus femoris at the anterior inferior iliac spine (Brukner & Khan 2007).
Occupation, sports, hobbies and lifestyle will certainly indicate the aggravating factors of the condition and allow the clinician to formulate a programme of treatment and advice, tailored to the patient’s individual needs.
Specific sports-related conditions should be considered. Stress fracture of the femoral neck may be encountered in young adults who are involved in endurance and high-intensity sports; initially anterior hip pain occurs late into the sporting activity but progresses to limit activity, occurring during any weight-bearing episode and even at rest. It should also be suspected in women with the female athletic triad of amenorrhoea, eating disorder and osteo-porosis. Diagnosis is essential to prevent progression to avascular necrosis of the femoral head (O’Kane 1999, Adkins & Figler 2000).
Osteitis pubis, a poorly understood pathological condition involving the pubic bone and symphysis pubis, presents with groin pain which may be bilateral. The symptoms may be aggravated by exercise, twisting, turning and kicking. Pain is provoked by resisted adduction (the ‘squeeze test’) which is usually accompanied by weakness, and there is tenderness to palpation over the pubic tubercles and symphysis pubis (Brukner & Khan 2007). The so-called ‘sports hernias’ should also be considered as a cause of anterior hip pain. These are thought to be responsible for activity-related hip pain, particularly in football, rugby and ice hockey players (O’Kane 1999). Inguinal hernia presents as a lump in the groin that goes away when the patient lies down. The lump reappears or increases on coughing and is not usually painful (Jenkins & O’Dwyer 2008). ‘Gilmore’s groin’ is not a hernia but should be considered in the differential diagnosis of groin pain, particularly in the sporting male. It is a disruption of the external oblique aponeurosis causing dilatation of the superficial inguinal ring, torn conjoined tendon and dehiscence between the inguinal ligament and the torn conjoined tendon (Williams & Foster 1995, Tibor & Sekiya 2008) (see p. 272).
The site and spread of pain may be local, indicating a superficial or less irritable lesion such as a muscle strain, or diffuse, indicating a larger lesion or gross inflammation.
Referred pain may originate from the lumbar spine. The sensory nerve supply to the hip joint is mainly through the femoral nerve L2–L3; therefore the joint itself refers pain into these dermatomes depending on the size of the lesion. Part of the L2 and L3 dermatomes covers the upper buttock and a hip lesion may present as low back pain only. Lesher et al (2008) looked at pain referral patterns arising from the hip joint. Of the 51 patients assessed, 55% of patients had referral to the groin and 57% to the thigh; 22% experienced pain in the lower limb distal to the knee, and occasionally to the foot, but the most common area for referral was buttock pain, experienced by 71% of patients. The most common referral combination was buttock pain with thigh referral, which occurred in 20% of subjects. This pattern of referral is similar to both the lumbar spine and sacroiliac joint and differential diagnosis can be difficult on the basis of pain referral alone. Other factors from the history and the objective examination will help towards clinical diagnosis and it is not unusual for the initial diagnosis to be modified following consideration of treatment outcomes.
Groin pain or pain referred to the knee in the child or adolescent without obvious cause must be considered serious and a specialist opinion sought for the possibility of the conditions mentioned above.
The onset of the symptoms may be gradual or sudden.
In osteoarthrosis the pain has a gradual onset, initially during weight-bearing activities, progressing to hip pain without weight-bearing, and present at rest (Cailliet 1990). A history of previous trauma such as fracture, which alters joint biomechanics, can predispose the joint to degenerative changes.
Relatively minor trauma can fracture the pelvis in the elderly, producing severe pain of sudden onset. Loose bodies present suddenly, as do traumatic muscular lesions. Muscles around the hip joint can be easily strained, since many are two-joint muscles, and a sudden explosive contraction such as that seen in sprinting may produce overstretching (Hartley 1995). Overuse or repetitive movements may produce chronic contractile lesions or bursitis.
The duration of symptoms indicates the stage of the lesion in the inflammatory process. Degenerative osteo-arthrosis will present a typical history of gradually worsening episodes of pain. Bursitis tends to give a gradual onset of aching pain and therefore is often present for many months before the patient seeks treatment. A severe pain which gradually increases in intensity, and remains so, is indicative of a serious lesion. This, coupled with other findings in the history, may be indicative of the ‘sign of the buttock’ (see p. 274).
The symptoms and behaviour need to be considered. The behaviour of the pain gives an indication of the nature of the lesion. For example, osteoarthrosis at the hip joint may be aggravated by activity or weight-bearing, or inflamed bursae and muscle sprains are worse with use and eased by rest.
The other symptoms described by the patient may give essential clues to diagnosis. Bursae produce pain on activities which squeeze or compress them, e.g. lying on the side or sitting. Loose bodies tend to produce twinging pain and a sensation of giving way on weight-bearing. Similar symptoms may be associated with labral tears or anterior acetabular chondral defects where clicking or locking may also be present (Neumann et al 2007). Arthritis tends to produce morning pain and stiffness due to accumulation of intracapsular swelling overnight (Hartley 1995). Degenerative osteoarthrosis, in its early stage, often produces night pain. Unrelenting pain should be considered serious, especially if the patient is unwell with a fever, night sweats and rigors.
To determine if the pain is coming from the lumbar spine, the patient is questioned about the presence of paraesthesia and pain produced by a cough or sneeze.
An indication of past medical history, other joint involvement and medications may give a clue to diagnosis and will establish whether contraindications to treatment techniques exist. Patients should be asked about any unexpected recent weight loss, indicative of more serious lesions, such as secondary deposits which are common in the hip and pelvis (Paice 1995). Differential diagnosis should also consider the exclusion of hip pain associated with pathology of the abdominal and pelvic organs as well as femoral or inguinal hernias. In addition to past medical history, establish any ongoing conditions and treatment. Explore other previous or current musculoskeletal problems with previous episodes of the current complaint, any treatment given and the outcome of treatment.
Inspection
An inspection of the general posture in weight-bearing will indicate any bony deformity. Look for general postural asymmetry which may be relevant, the position of the buttock creases, posterior superior iliac spines, anterior superior iliac spines, level of the iliac crests, any leg length discrepancy and the position of the feet.
Colour changes and swelling are not expected at the hip because it is such a deep joint, but they may be associated with trauma, bruising and abrasions. If redness and swelling are present in the buttock area without a history of trauma, the ‘sign of the buttock’ (see p. 274) may be suspected.
Muscle wasting may be seen in the glutei associated with a lumbar lesion, or in the quadriceps associated with degenerative osteoarthrosis of the hip or a lumbar lesion.
State at rest
Before any movements are performed, the state at rest is established to provide a baseline for subsequent comparison.
Examination by selective tension (objective examination)
The suggested sequence for the objective examination will now be given, followed by a commentary including the reasoning in performing the movements and the significance of the possible findings. Comparison should always be made with the other side.
Eliminate the lumbar spine
• Extension repeated with foot on stool if indicated (Fig. 10.7)
 |
| Figure 10.7 Active extension with hip flexed to differentiate between hip and lumbar spine as the cause of pain. |




Supine lying









Prone lying







Accessory test for the psoas bursa
• Passive hip flexion and adduction (Fig. 10.28)
 |
| Figure 10.28 Combined flexion and adduction to compress the psoas bursa. |
Accessory test for the ‘sign of the buttock’
• Straight leg raise (Fig. 10.29)
 |
| Figure 10.29 Straight leg raise, accessory test for ‘sign of the buttock’. |
Palpation
• Once a diagnosis has been made, the structure at fault is palpated for the exact site of the lesion
The routine for the examination of the hip is conducted in the above order as it allows all tests in each position of standing, supine and prone to be completed.
The lumbar spine is first assessed by the four active movements. If active lumbar extension reproduces the pain, it should be repeated with the hip joint eliminated by placing it into flexion with the foot up on a stool. If extension is still painful, the lesion lies in the lumbar spine and a more thorough investigation of this must then be made. The straight leg raise and femoral stretch tests are applied within the examination sequence to test for neural involvement. The straight leg raise does stretch the hamstrings, which needs to be considered within clinical reasoning, and is part of an accessory test to look for serious pathology in the hip or pelvis (see below).
Related posts:






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


