Chapter 6 The Elbow
The elbow is a strong hinge joint that allows flexion and rotation of the forearm. It also provides the bony origin for most of the extrinsic muscles of the wrist and hand. It is frequently affected by inflammatory and traumatic conditions that seriously alter its function. Osteoarthritis is rare, however.
Anatomy
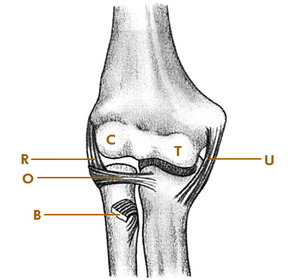
The elbow joint is formed by the articulation between the humerus and the radius and ulna (Fig. 6-1). The humerus widens distally to form the lateral and medial condyles. The capitellum of the lateral condyle articulates with the radial head, and the trochlea articulates with the ulna. The head of the radius also articulates with the lateral aspect of the ulna and is held in position by the orbicular ligament. Medial and lateral collateral ligaments provide additional stability.
Examination
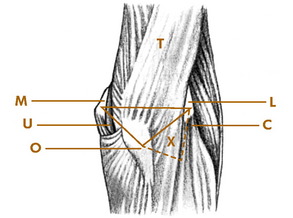
The tip of the olecranon process and the epicondyles form useful bony landmarks (Fig. 6-2). When the elbow is fully extended and viewed from behind, these points form a straight, transverse line. With the elbow flexed, they form an isosceles triangle. Just distal to the lateral epicondyle lies the radial head. These two points, along with the olecranon process, form another triangle on the posterolateral aspect of the joint. This triangle is occupied by the anconeus muscle. This area usually bulges when the joint is distended by fluid and is an excellent site for joint aspiration.
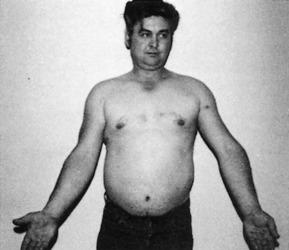
With the forearm in the supinated position, an angle is formed with the arm at the elbow joint. This is referred to as the “carrying angle” and normally measures 15 to 20 degrees. Alterations in this angle may occur following injury or infection, especially in the young, and may lead to excessive cubitus valgus or even varus (Fig. 6-3).
Roentgenographic Anatomy
The roentgenographic features of the elbow are well visualized by standard anteroposterior and 90-degree flexion lateral views (Fig. 6-4). Comparison views of the opposite elbow should be obtained whenever necessary. Oblique views are helpful when the diagnosis is uncertain.

Epicondylitis
Epicondylitis is one of a large group of musculoskeletal disorders commonly termed “overuse syndromes.” Although it is often called an inflammatory condition, degeneration (tendinosis) is usually present instead, often with the development of local neovascular tissue. The condition is characterized by pain at the origin of the flexor muscles at the medial epicondyle or the extensor muscles at the lateral epicondyle. Some cases may start with a direct blow, but the cause is usually unknown. Minor tears in the tendinous attachments of these muscles are often present. The disorder is common in individuals whose activities require repeated use of the extensor or flexor mechanism of the forearm. The lateral side (“tennis elbow”) is more commonly involved. In tennis players, the backhand swing seems to be the main offender. Involvement of the medial epicondyle is often called “golfer’s elbow.”
CLINICAL FEATURES
The onset is usually gradual. A dull ache that worsens with use of the involved muscles appears over the affected epicondyle. Palm-down lifting is painful. Activities that require rotation and grasping, such as opening a jar, increase the pain. The pain often radiates into the forearm. Extension or flexion of the hand against resistance reproduces the pain at the affected epicondyle (Fig. 6-5). The point of maximum tenderness can usually be well localized by digital pressure applied about 1 cm distal to the epicondyle. The roentgenograms are usually normal, although a traction spur or calcification may be present.

TREATMENT
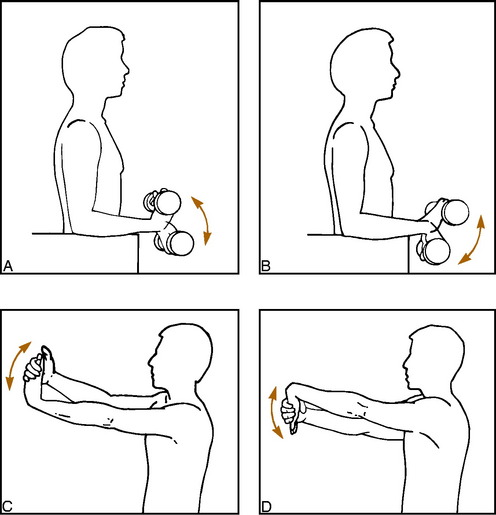
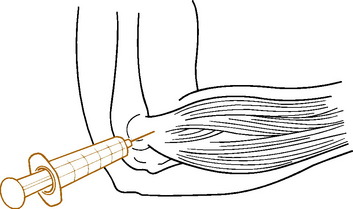
Treatment is similar to that for other “musculotendinous overuse syndromes.” Rest is important, and this can frequently be obtained merely by avoiding the offending activity. Applying ice after exercise can help. A careful exercise program of gentle stretching and strengthening is begun as pain subsides (Fig. 6-6). Nonsteroidal anti-inflammatory drugs (NSAIDs) are given as necessary. Local infiltration of the affected area with 1 to 2 mL of a steroid/lidocaine mixture often provides permanent or at least long-lasting relief (Fig 6-7). The injection is placed in the area of maximum local tenderness, usually about 1 cm distal to the bony epicondyle, and may be repeated two or three times. A tennis elbow counterforce strap may also be tried. It theoretically works by dampening the force transmitted to the elbow from the hand and wrist (see Chapter 15). Extracorporeal shock wave therapy (ESWT) has even been tried in epicondylitis, but the results are inconclusive. The disease is usually self-limited, but symptoms may persist for several months before full recovery. Conservative treatment is effective in most cases. Often, spontaneous rupture of the aponeurosis probably occurs, which cures the pain, usually without any significant residual weakness. Surgery is reserved for cases that do not respond to medical management. Eventually, the recreational tennis player may simply have to decide to withdraw from the sport.
Osteochondritis Dissecans
Osteochondritis dissecans is a condition in which a portion of subchondral bone undergoes avascular necrosis. This segment of bone, with its overlying articular cartilage, may partially or completely separate from the adjacent bone and even extrude into the joint to form a loose body. The disorder is most commonly seen in the knee joint, but a similar condition also occurs in the elbow, ankle, and hip joints. The cause is unknown, but it is probably traumatic in origin. Repetitive compression of the lateral elbow joint may be responsible. The condition is sometimes a cause of “Little League elbow.”
CLINICAL FEATURES
In the elbow, the disorder is most common during adolescence, and males are usually affected. The onset of symptoms is gradual, and a history of trauma may be elicited. The patient frequently complains of a dull, aching pain that is often associated with stiffness. Occasionally, episodes of locking occur if the fragment has become extruded into the joint. The physical findings consist of limitation of motion, local tenderness, and joint effusion. Roentgenographically, the capitellum is the most common site of involvement (Fig. 6-8).

Pronator Syndrome
The median nerve gives off its motor branch, the anterior interosseous nerve, below the elbow as it passes between the two heads of the pronator teres muscle just behind the biceps aponeurosis. An uncommon form of compression neuropathy can occur at this site, which is called pronator syndrome. Entrapment can also cause a very specific clinical presentation, sometimes referred to as the anterior interosseous nerve syndrome if only the motor branch is affected. The etiology is usually some form of localized anatomic compression, but the disorder can follow injury or even a traumatic phlebotomy.






Stay updated, free articles. Join our Telegram channel

Full access? Get Clinical Tree


